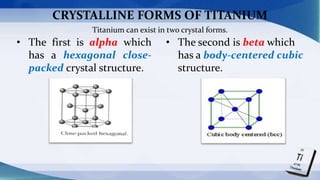
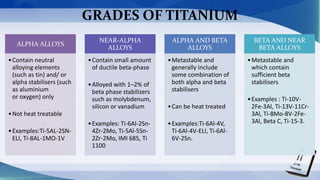
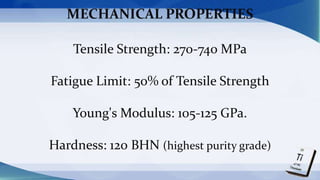
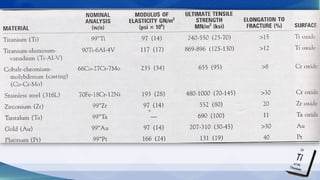
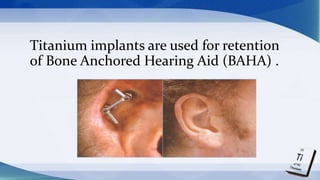
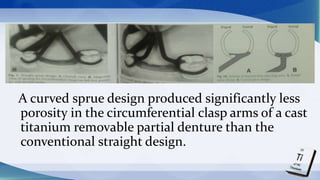
Titanium alloys have various clinical applications in dentistry due to their high strength, light weight, corrosion resistance, and biocompatibility. Titanium can be used for removable partial denture frameworks, complete dentures, implant abutments, fixed partial dentures, and maxillofacial prostheses. Titanium exists in two crystalline forms and various grades suitable for different applications. Special casting and machining techniques must be used to process titanium due to its high reactivity and potential to form surface oxides. Low-fusing porcelains and special protocols are required for veneering titanium fixed partial dentures.