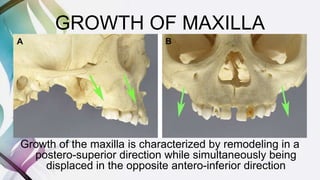
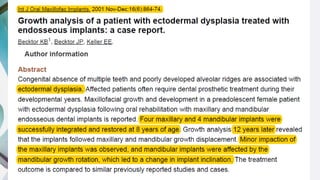
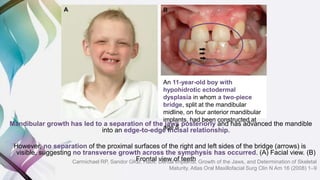
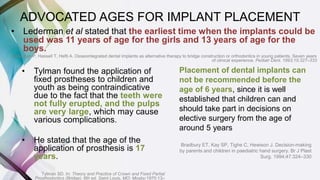
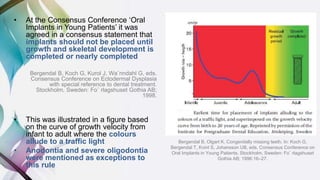
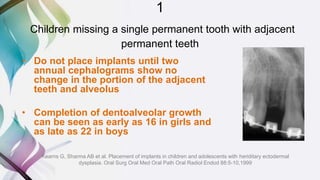
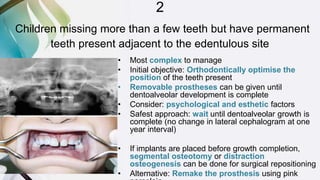
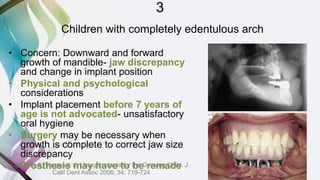
This document discusses the use of dental implants for growing patients. It outlines concerns about implant placement interfering with jaw growth and tooth eruption. Case reports show implants becoming submerged or misaligned due to residual growth. The youngest child reported with implants was 1.5 years old. Recommendations include not placing implants before age 6, and waiting until growth is nearly complete, usually around 17 years old. Exceptions may be made for patients with complete anodontia. Regular prosthesis adjustments are needed to account for jaw growth.





















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










