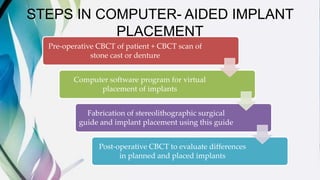
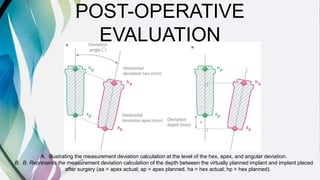
This document summarizes a review of the accuracy of computer-aided implant placement. It finds that on average, implants placed using guided surgery techniques deviated 1.09mm at the entry point, 1.28mm at the apex, and 3.9 degrees in angulation compared to virtual planning. Some studies found greater accuracy in the mandible versus maxilla and in anterior versus posterior regions. Potential advantages of guided flapless surgery include reduced pain, swelling and treatment time, while common complications are surgical guide fracture and implant failure rates of 3-10%. The review concludes that more randomized controlled trials are needed but current evidence supports the accuracy of computer-guided implant placement.


























































![NEW dental implant design [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/newimplantdesignautosaved-250614065418-013f8c1f-thumbnail.jpg?width=640&height=640&fit=bounds)




























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


