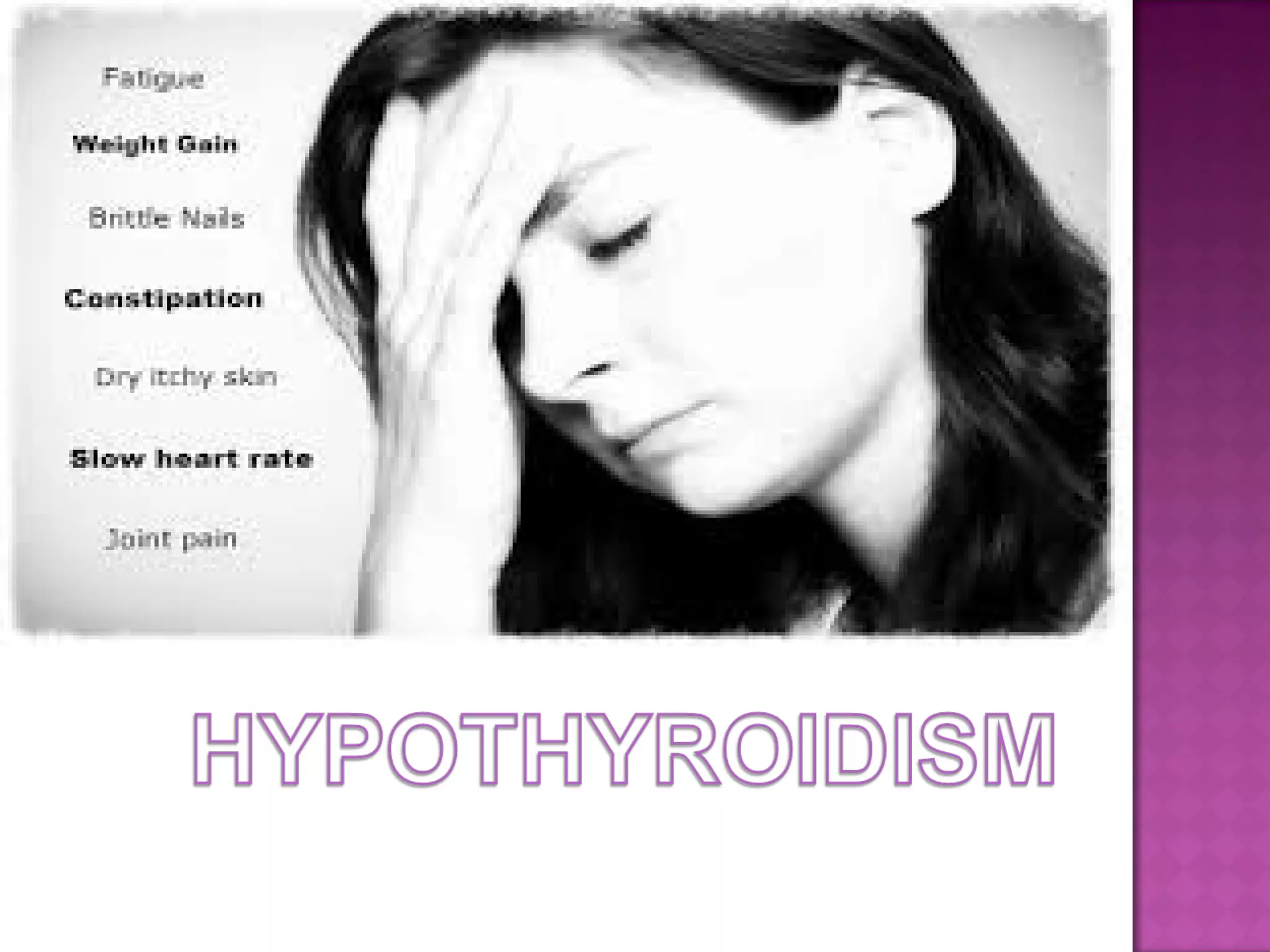
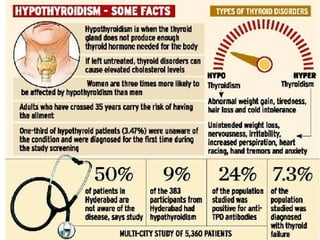
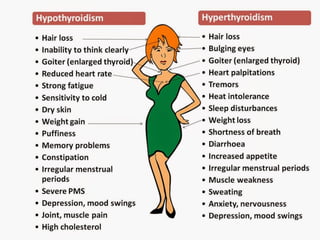
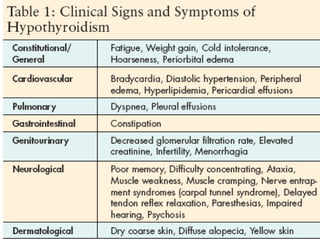
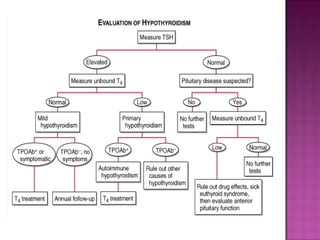
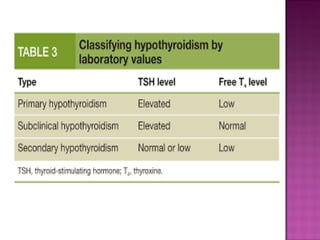
This document discusses causes and symptoms of hypothyroidism. It begins by listing primary causes such as autoimmune disorders, iatrogenic causes from medical treatments, drugs that can cause it, and congenital issues. It then discusses signs and symptoms, focusing on tiredness, dry skin, cold sensitivity, hair loss, cognitive issues, and weight gain being most common. It also describes autoimmune hypothyroidism in more depth, covering genetics, pathogenesis, clinical features in adults and children, diagnosis and testing.