Downloaded 119 times





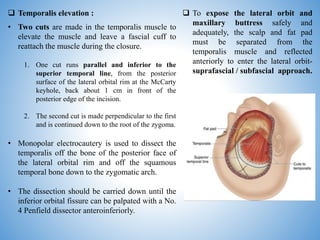










The document describes the frontotemporal orbitozygomatic (FTOZ) craniotomy surgical approach. It discusses the key anatomical landmarks and surgical steps involved in the approach. The FTOZ approach provides exposure of the parasellar region, anterior circulation aneurysms, and lesions of the cavernous sinus. It can be performed as a one-piece, two-piece, or three-piece craniotomy. Important tips include protecting the superficial temporal artery and periorbita during dissection and osteotomies.













































![[19330693 - Journal of Neurosurgery] Transorbital endoscopic amygdalohippocam...](https://cdn.slidesharecdn.com/ss_thumbnails/19330693-journalofneurosurgerytransorbitalendoscopicamygdalohippocampectomyafeasibilityinvestigation-240717053318-9fb04df5-thumbnail.jpg?width=640&height=640&fit=bounds)









































