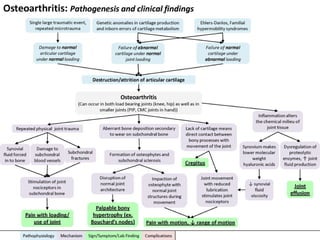
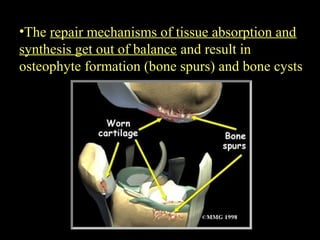
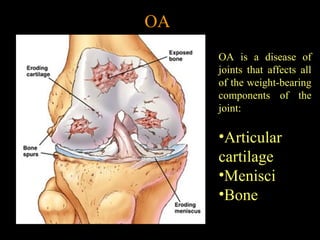
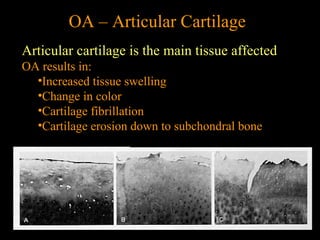
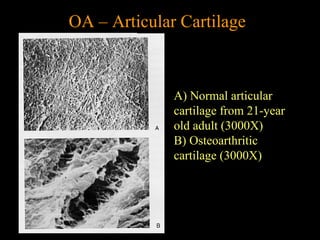
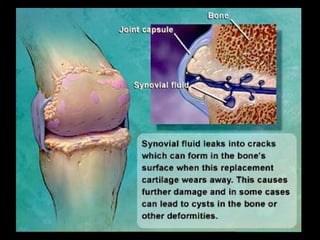
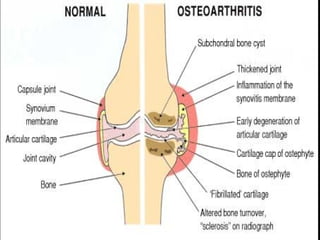
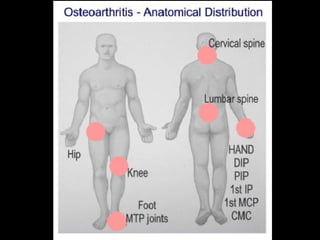
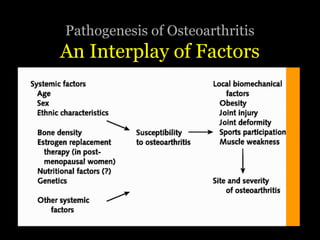
Osteoarthritis is the most common form of arthritis that affects the joints, especially in those over 45 years old. It involves the breakdown of cartilage in the joints which leads to pain, stiffness, and reduced mobility. Risk factors include age, genetics, joint injuries, and obesity. Symptoms may include joint pain, stiffness, swelling, and grinding sensations. Diagnosis involves physical exams, x-rays showing cartilage loss and bone spurs, and ruling out other causes. Treatment focuses on reducing pain and inflammation with medications and physical therapy, as well as weight loss and joint protection. For severe cases, surgical options like joint replacement may be considered.

![OA – Symptoms
• OA usually occurs slowly -
It may be many years before
the damage to the joint
becomes noticeable
• Only a third of people
whose X-rays show
OA report pain or
other symptoms:
– Steady or intermittent pain in a joint
– Stiffness that tends to follow periods of inactivity, such as sleep
or sitting
– Swelling or tenderness in one or more joints [not necessarily
occurring on both sides of the body at the same time]
– Crunching feeling or sound of bone rubbing on bone (called
crepitus) when the joint is used](https://image.slidesharecdn.com/osteoarthritis-170618093018/85/Osteoarthritis-22-320.jpg)