INTRODUCTION
• Neural tubedefects (NTDs) are birth defects (congenital
conditions) of the brain, meninges or spinal cord.
• Occur to developing fetuses within the first month of pregnancy
(3rd
4 OR 5 $6 week of pregnancy)
• Often before a mother knows she is pregnant.
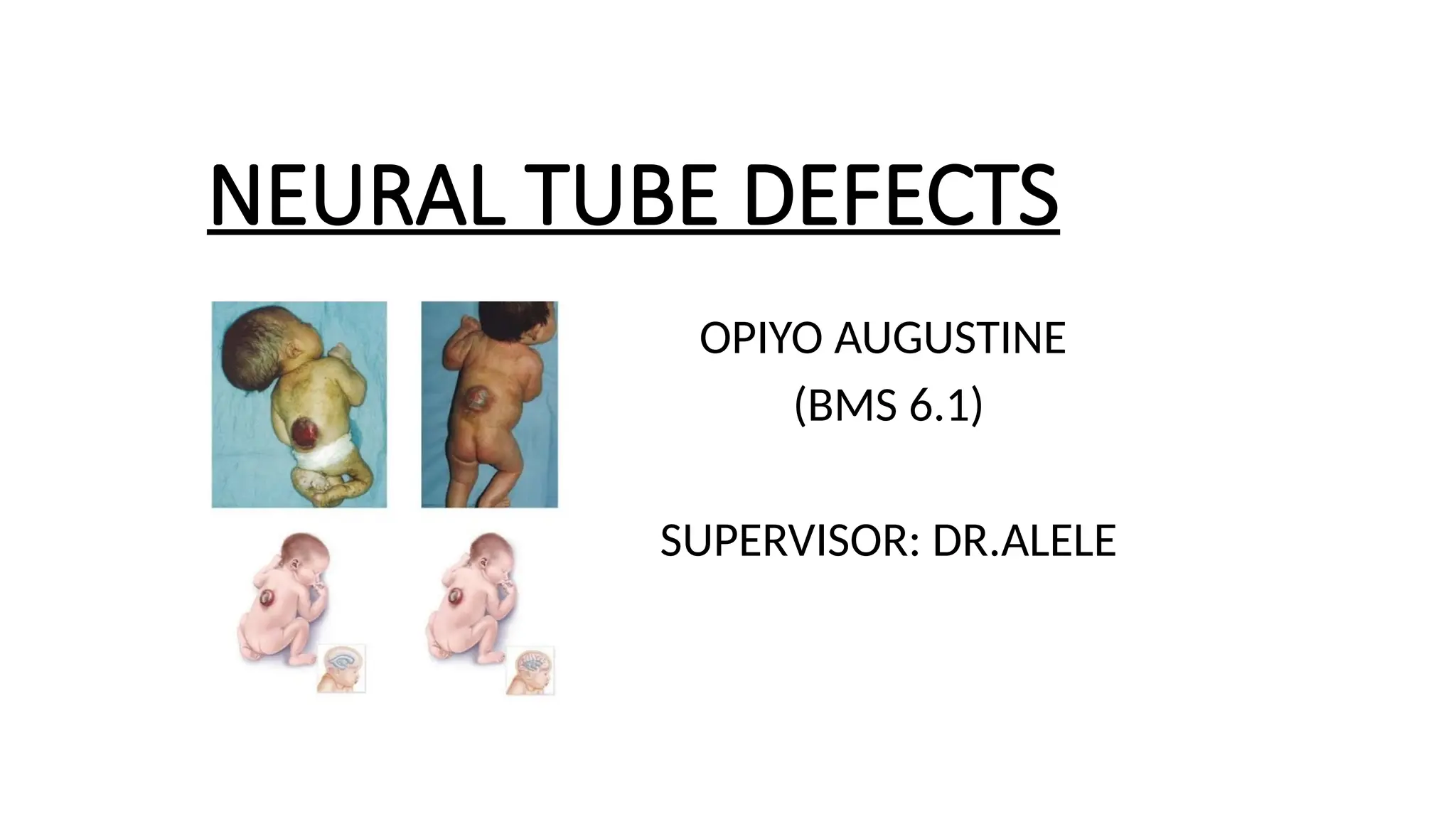
• The two most common neural tube defects are Spina bifida and
Anencephaly.
4.
EPIDEMIOLOGY
• The prevalenceof NTDs ranges from one to 10 per 1,000 births,
being highest in some regions of China.
• In Africa: 11.7 per 10,000 live births
• Spina bifida in Africa was 0.13% with a range between 0.12% and
0.14%.
• In Africa, the highest burden of Spina bifida was detected in
Algeria (0.43%), Ethiopia (0.32%), Tanzania (0.26%), Cameron
(0.12%), Egypt (0.10%), and South Africa (0.10%).
• Eastern Africa is 5 times as high as observed in Western countries
(Third world countries > developed countries)
5.
RISK FACTORS
Exact causeof NTDs are unknown, but associated with the following
factors;
• Genetical factor + Ethnicity (Indians > Whites)
• Nutritional factor especially Folic acid deficiency-B9
• Environmental factor e.g. toxicants, pollutants, radiations
• Intake of anti epileptic medication during pregnancy or before
that interfere with folate metabolism
• Obesity that accelerated the condition
• Diabetes (insulin dependent) poorly controlled
(less folate may find its way to the developing fetus)
6.
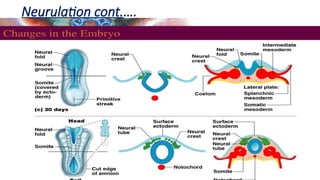
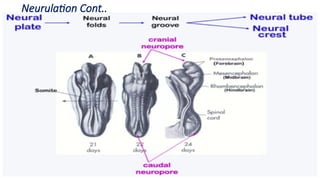
EMBRYOLOGY
• Neurulation isthe process that leads to the development of the
CNS starting around 21 days post fertilization in humans and
involves the folding process in vertebrate embryos causing
transformation of the neural plate into the neural tube.
• The neural tube is the primordium (structure in earliest
development) of the meninges, brain and spinal cord.
• (Neural ectoderm forms to form 2 ends and this process peaks on
day 21 )
• A neuroporeis formed when the middle portion fuses and the caudal and cranial
ends are not fused
• The neurotube consists of ;
1.Anterior neuropore : Anterior / Cranial half. Usually closes at day 25
2.Posterior neuropore : Posterior / Caudal half. Usually closes at day 28
• Closure usually occurs in the first month of pregnancy
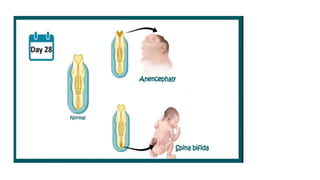
PATHOGENESIS
Failure of theneural tube to close leads to;
• Spina bifida results from incomplete closure of the neural tube at
the caudal end (most commonly in the lumbar region). Also
known as Spinal cord defect
• Anencephaly results from failure of the neural tube to close at the
cephalic end, leading to the partial absence of the brain and skull.
Rarely survives. Also known as brain defect.
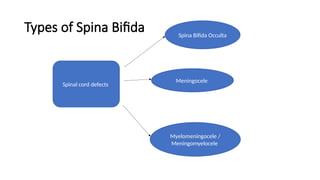
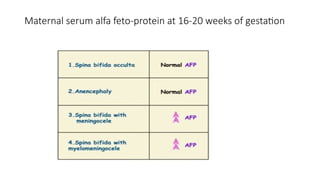
TYPES OF SPINABIFIDA
Spina bifida occulta:
• Is the least severe but most common
• Have a small gap in the Spine but the opening cannot be seen
in the back.
• Usually presents with a Taft of hair on dorsal region, dimple or
birthmark above the site of the lesion
• Brain and spinal cord functions are normal and there is no
disabilities.
• No protrusion of spinal cord or tissue
• It usually discovered only on x ray or CT scan as an incidental
finding
OCCULTA CONT’D
• Either1 or more vertebrae may be malformed or missing from
development
• Not usually diagnosed, is of low consequences
• Occulta mean Hidden and is therefore not easily caught on
prenatal tests
18.
MENINGOCELE / MENINGEALCYST
• Is a sac of fluid (not involving the spinal cord) that herniates
through an opening in the back and involves meninges also.
• May or may not be covered by skin.
• Presents with minor symptoms since spine is not damaged.
• Usually has a glowing / shining appearance
• They may present with symptoms such as low back pain and
bowel and bladder symptoms
MYELOMENINGOCELE / MENINGOMYELOCELE
•Is one of the most common and most severe form of Spina bifida.
• The unfused portion of the spinal column allows the spinal cord to protrude through an
opening
• Forming a sac enclosing the spinal elements, such as;
1. Meninges
2. Cerebrospinal fluid
3. Parts of the spinal cord and nerve roots
MYELOMENINGOCELE CONT’D
• Theskin may or may not be present
• The nerves protrude and exposed (Open Spina Bifida)
• Dorsal arch not fused (Mesoderm fail to organize over defect)
• Increased chance of infections : Meningitis, renal problems
• Associated with Arnold Chiari II Malformation: Cerebellar +
Brainstem tissue slips down into foramen magnum (Opening of the
base of the skull) causing changes in brain structures
23.
Signs and symptoms
•Loss of bladder or bowel control (Neuropathic bladder and bowel)
• Partial or complete loss of sensation
• Partial or complete paralysis of the legs below damaged site
• Weakness of the hips, legs, or feet of a newborn
• Seizures
Others;
1. Clubfoot
2. Hydrocephalus
3. Hair present at the sacral region
4. Dimpling of the sacral area
24.
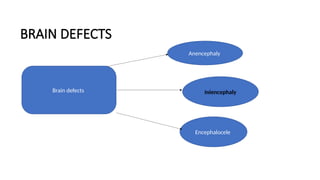
BRAIN DEFECTS
Anencephaly;
• Isthe absence of a major portion of the brain, skull and scalp that
occurs during embryonic development.
• Infant with this disorder do not survive longer than a few hours or
possibly days after their birth.
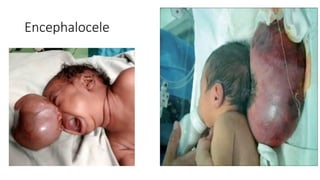
ENCEPHALOCELE
• Sometimes knownas cranium bifidum
• Is a NTD characterized by sac like protusions of the brain and
meninges and membranes that cover it (through an opening in
the skull)
Symptoms;
1. Neurologic problems
2. Hydrocephalus
3. Spastic quadriplegia : Weak and inactive muscles
4. Microcephaly
CRANIORACHISCHISIS / RACHISCHISIS
• Extreme form of neurotube closure defect
• Absence of brain and cranial vault without skin covering , with
bony defect of cervical spine due to failed fusion of the dorsal
arch and no closure of the spinous process
1.Vertebrae remains open
2.SC and meninges herniate outside
3.CSF leaks outside
MANAGEMENT
Medical care;
• Thepatient should be positioned in prone position to prevent
pressure on the defects
• The newborn with an open NTD should be kept warm and the
defects covered with a sterile wet saline dressing.
• Prophylactic IV antibiotic should be initiated.
36.
MANAGEMENT CONT’D
Surgical;
• Neurosurgicalrepair of the defects is considered the mainstay of
treatment for open Spina bifida.
• Closed Spina bifida does not usually warrant any immediate
surgery.
• The closure is typically performed within 1 to 3 days after delivery
to minimize the risk of infections.
• Neonate born with severe Hydrocephalus should have
ventriculoperitoneal shunt placed concurrently.
37.
Nursing interventions
• Evaluatethe sac and measure lesion
• Monitor for increased ICP
• Measure head circumference
• Protect sac with non adherent moist dressing
• Place child in prone position
38.
Nursing interventions cont.…
•Use aseptic techniques
• Monitor for early signs of infection
• Administer antibiotics
• Prepare family for surgery
39.
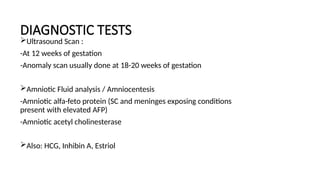
PREVENTION OF NTDs
•All women of childbearing age should take a daily supplement of
400 micrograms of folic acid.
• Educate mothers regarding intake of folic acid especially in the
preconception period and during pregnancy
• Women who already had first pregnancy with NTDs should take a
daily 4mg tablet of folic acid for at least one month before
conception and then throughout the first 12 weeks of pregnancy.
• Genetic counseling or screening
• Use fortified breakfast cereal and flour
40.
REFERENCES
• Roberts, Iwan.“Nelson’s textbook of pediatrics (20th
edn.), by R.
Kliegman, B. Stanton, J. St. Geme, N. Schor (eds) Elsevier,
Philadelphia, 2016, Hardcover (2 volumes) 3,888 pp., English,
ISBN 978-1-4557-7566-8
• https://scholar.google.com/scholar?
hl=en&as_sdt=2005&sciodt=0%2C5&as_ylo=2022&cites=1583528
3910122670520&scipsc=&q=incidence+of+neural+tube+defects+i
n+Africa+&btnG=#d=gs_qabs&t=1680633098619&u=%23p
%3DYQZIwMaXgj8J










































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















