Download as PDF, PPTX
















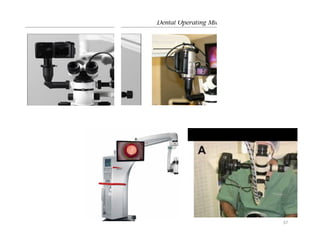












































This document discusses the use of surgical microscopes in endodontics, detailing their history, optical principles, parts, clinical applications, and advantages over traditional methods. The introduction of these microscopes has significantly improved the ability to visualize and treat complex dental issues, enhancing safety and effectiveness in both nonsurgical and surgical procedures. It also addresses various types of magnification techniques, positioning, ergonomics, and care for the equipment.















































![Microscopes 1[1]/ orthodontic course by indian dental academy](https://cdn.slidesharecdn.com/ss_thumbnails/microscopes11-140427071202-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)







































