Downloaded 54 times
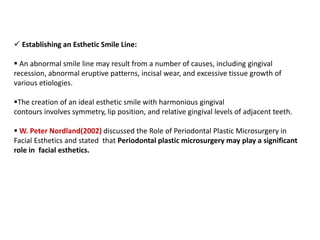
![Periodontal regeneration
Several authors have proposed the use of microsurgical approach for the treatment of
isolated[Wachtel H et al., 2003, Cortellini P et al., 2007, Jepsen S et al., 2008, Cortellini P
et al., 2009] or multiple intrabony defects. (Harrel SK et al.,2005, Cortellini P et al 2008.)
The advantages of microsurgical approach in regenerative therapy relate to improved
illumination and magnification of the surgical field that permits proper access to and
debridement of the intrabony defect with an increased accuracy and minimal trauma.
Cortellini P, Tonetti MS., 2007](https://image.slidesharecdn.com/periodontalmicrosurgery-200819132717/85/Periodontal-microsurgery-33-320.jpg)

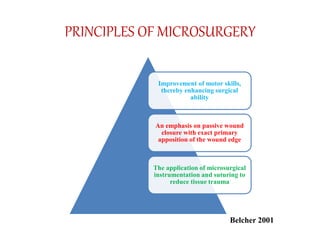
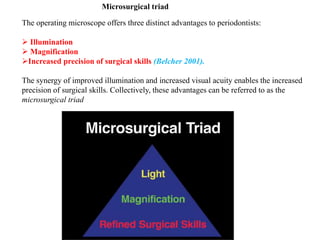
This document provides an overview of periodontal microsurgery. It discusses the history and development of microsurgery, principles of microsurgery including the microsurgical triad of illumination, magnification, and precision. It describes different types of magnification systems including loupes and surgical microscopes and their advantages and limitations. The document outlines indications for periodontal microsurgery and discusses microsurgical instruments and principles of ergonomics. It concludes that periodontal microsurgery utilizes improved visualization to allow for more precise surgical techniques.






























![MIST[1bhjjkkklll do by Jo or ah nu].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mist1-250525215919-08871855-thumbnail.jpg?width=640&height=640&fit=bounds)




































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)













