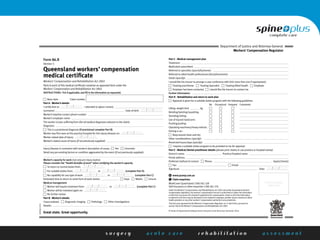
This document provides guidance for medical practitioners on completing workcover medical certificates. It addresses key areas such as documenting diagnoses, assessing work capacity and rehabilitation plans. Practitioners are advised to consider the health benefits of work when certifying capacity, provide clear work restrictions, and identify barriers to timely return to work in order to facilitate claim processing. Confidentiality and obtaining appropriate consent for information sharing with insurers is also discussed.