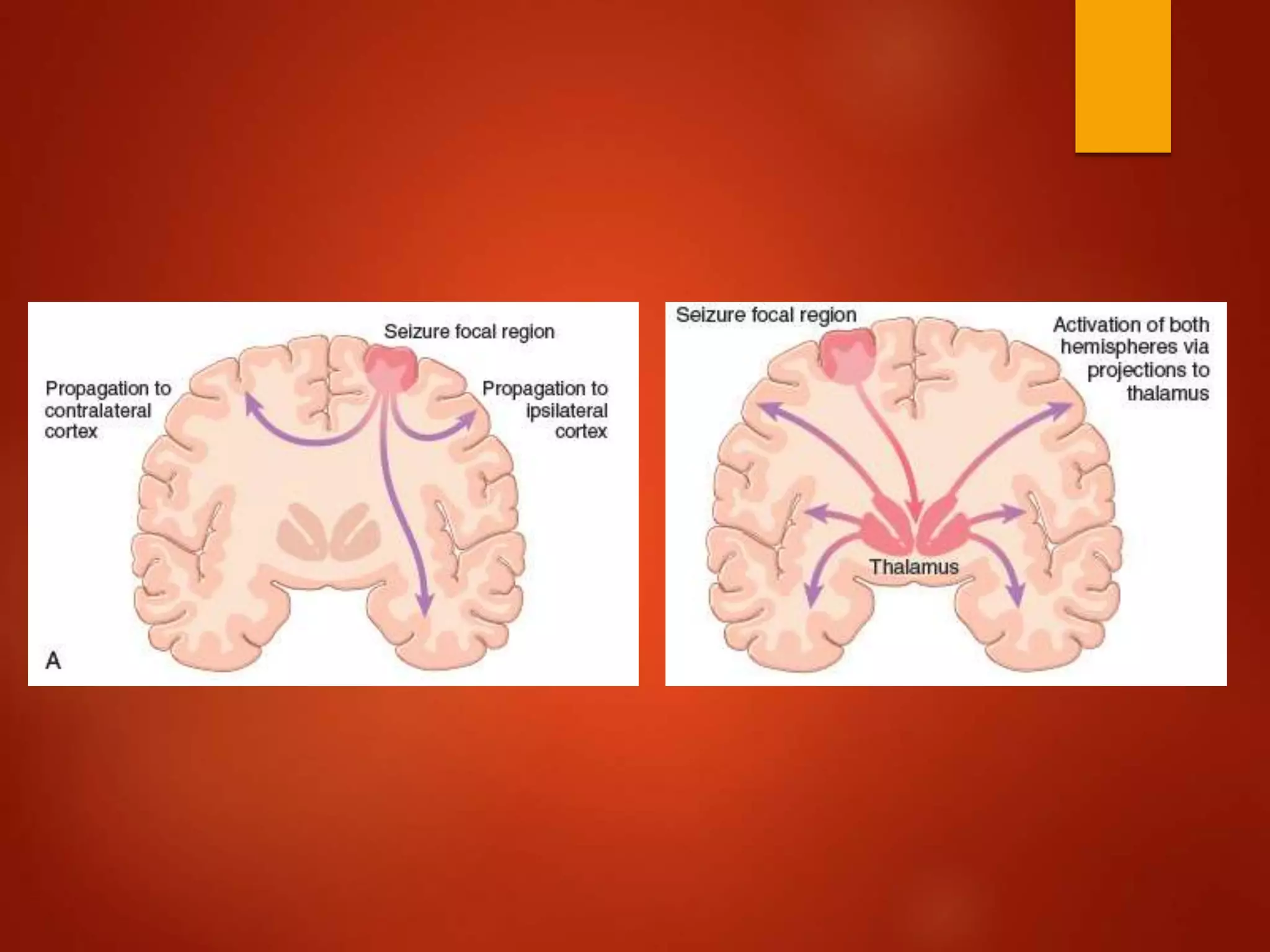
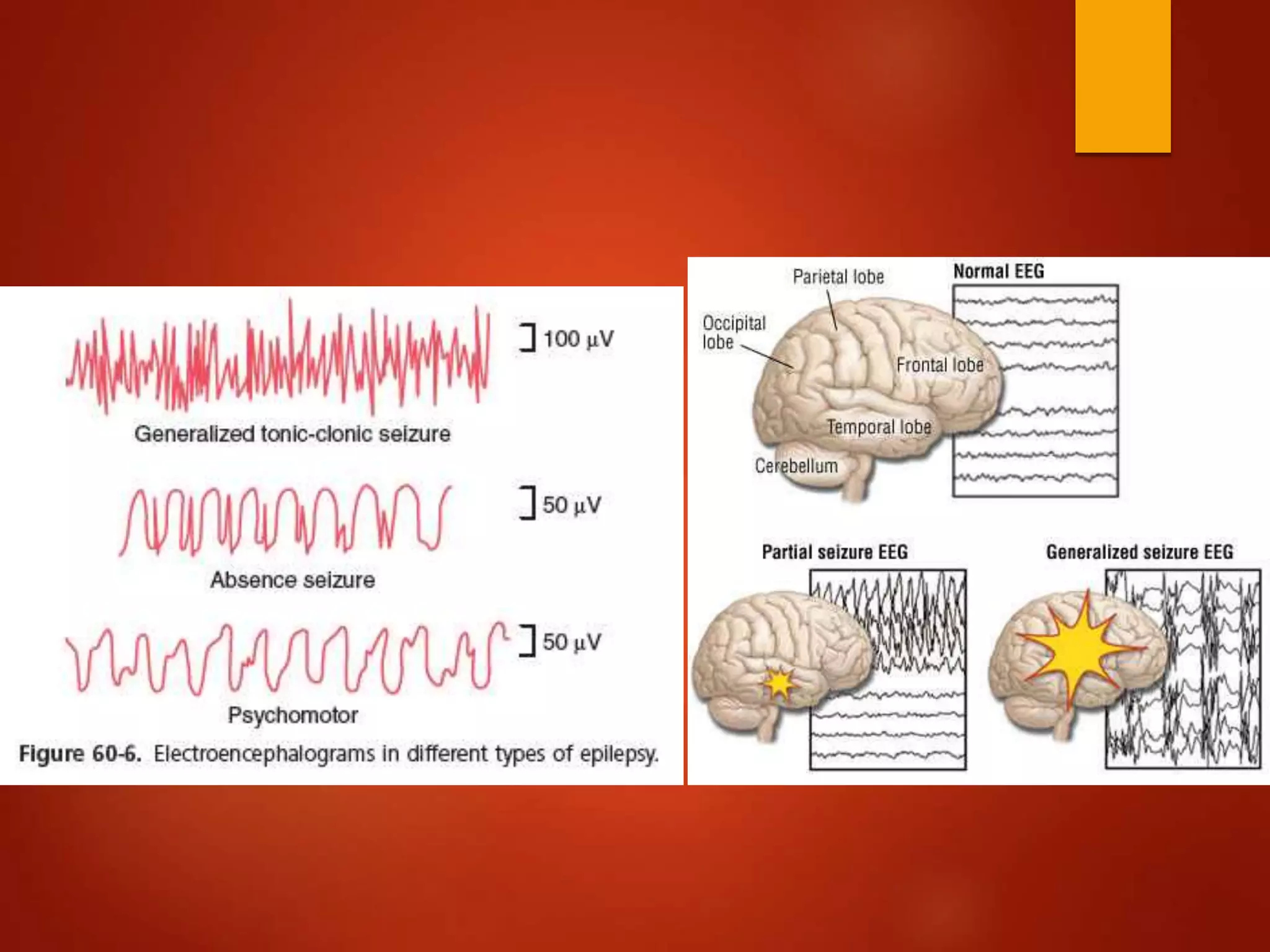
Epilepsy is a chronic condition characterized by recurrent seizures caused by excessive neuronal activity in the brain. Seizures occur when clusters of neurons fire abnormally, driven primarily by glutamate and its NMDA receptor. Some people have genetic mutations affecting the GABA receptor, reducing inhibition of neuronal signals. Seizures can be focal, originating in one brain region, or generalized across both hemispheres. Focal seizures may or may not impair consciousness. Generalized seizures include tonic, clonic, myoclonic, absence and tonic-clonic types. Diagnosis involves tests like MRI, CT and EEG to identify potential causes. Treatment options include anticonvulsant drugs, epilepsy surgery, nerve stimulation, and























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)