Downloaded 126 times

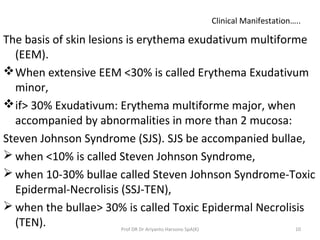
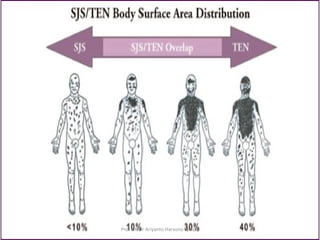


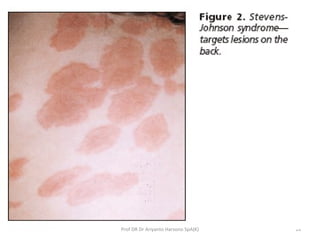






Steven-Johnson syndrome (SJS) is a severe skin reaction typically caused by drug reactions. It is characterized by painful sores and blisters in the mouth, eyes, and other mucus membranes. SJS progresses to toxic epidermal necrolysis (TEN) when over 30% of the skin is affected and shows widespread damage. Both SJS and TEN can cause blindness, infection, and death if not properly treated with fluid replacement, antibiotics, steroids, and stopping the causative drug. Prompt diagnosis and management are important to prevent complications and improve prognosis of these potentially life-threatening conditions.















































![STEVEN JOHNSONS SYNDROME AND TOXIC EPIDERMAL NECROLYSIS [Autosaved] 2.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/stevenjohnsonssyndromeandtoxicepidermalnecrolysisautosaved2-250619172417-940965c8-thumbnail.jpg?width=640&height=640&fit=bounds)











![dermatological emergencies [Autosaved] [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dermatologicalemergenciesautosavedautosaved-250718141557-4ff0fe21-thumbnail.jpg?width=640&height=640&fit=bounds)





