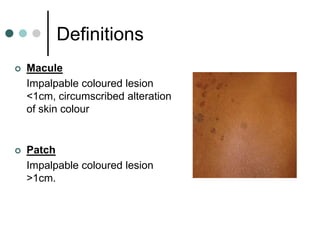
This document defines common skin conditions and provides guidance on evaluating dermatology presentations in the emergency department. It reviews terminology, discusses common non-serious conditions like urticaria and eczema, and outlines serious but rare disorders involving blistering or skin loss such as erythema multiforme major, pemphigus, pemphigoid, and toxic epidermal necrolysis. Red flags are identified that warrant discussion with a senior colleague or dermatologist.




































![1.1.2. viral infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-2-viralinfectionsofskincompatibilitymode-120714004456-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)









































































