Downloaded 504 times




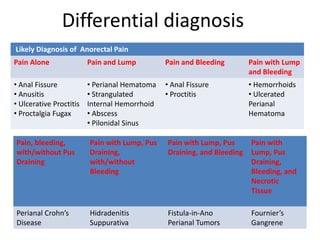




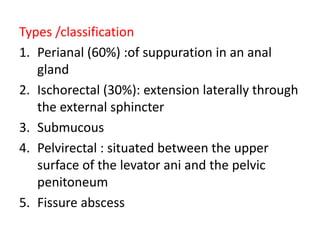


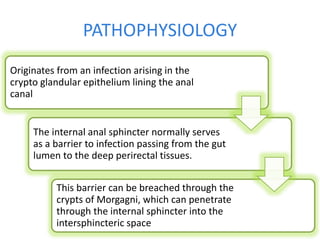







This presentation discusses the diagnosis and management of anorectal abscesses. Key points include: - Anorectal abscesses typically present with perianal pain, swelling, and drainage and are usually caused by a cryptoglandular infection. - Differential diagnoses depend on associated symptoms and may include hemorrhoids, fistulas, or Crohn's disease. - Evaluation involves examination, blood tests, and imaging studies. - Treatment is early surgical drainage of the abscess to prevent complications like fistula formation or impairment of sphincter function. Postoperative care involves antibiotics, pain relief, and follow-up to monitor for healing or complications.























































































