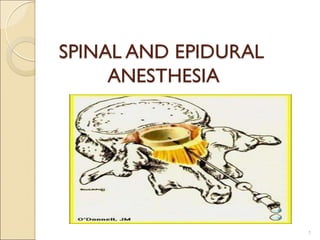
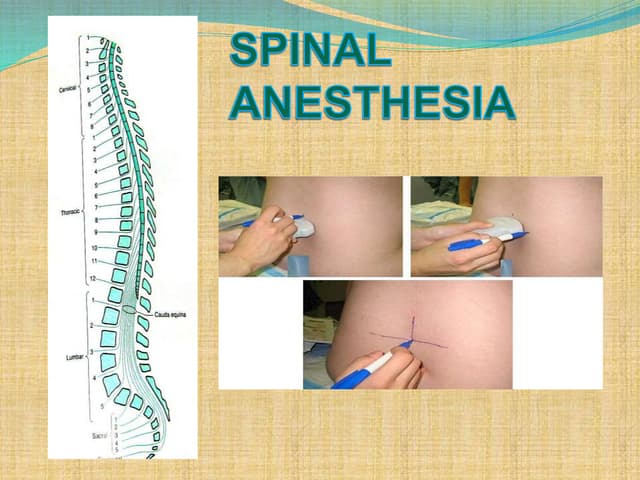
This document discusses spinal anesthesia, including its definition, advantages, indications, contraindications, how to perform it, and potential complications. Spinal anesthesia involves injecting local anesthetic into the cerebrospinal fluid below L2 to anesthetize the lower body. It has advantages like low cost, patient satisfaction, and reduced risk of complications. Indications include lower abdominal and genitourinary surgeries. Contraindications include coagulation disorders and hypovolemia. Performing it requires cleaning the back, locating an interspinous space, and slowly injecting anesthetic when cerebrospinal fluid is seen. Complications can include hypotension, headache, and urinary retention.