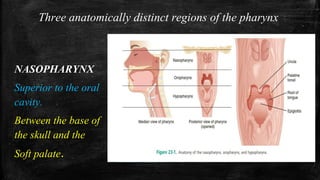
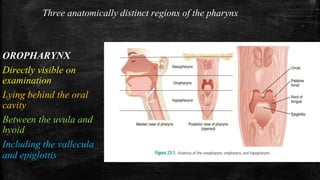
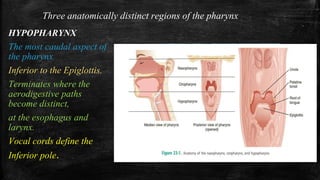
The document discusses the evaluation and management of sore throat. It begins by describing the three anatomical regions of the pharynx - nasopharynx, oropharynx, and hypopharynx. The diagnostic approach involves airway assessment, examination of the pharynx, and using the Centor criteria to determine if pharyngitis is likely viral or bacterial. Empirical management focuses on pain control, corticosteroids, drainage of peritonsillar abscesses, and antibiotics only in specific cases rather than routinely for pharyngitis which is usually self-limiting and viral.