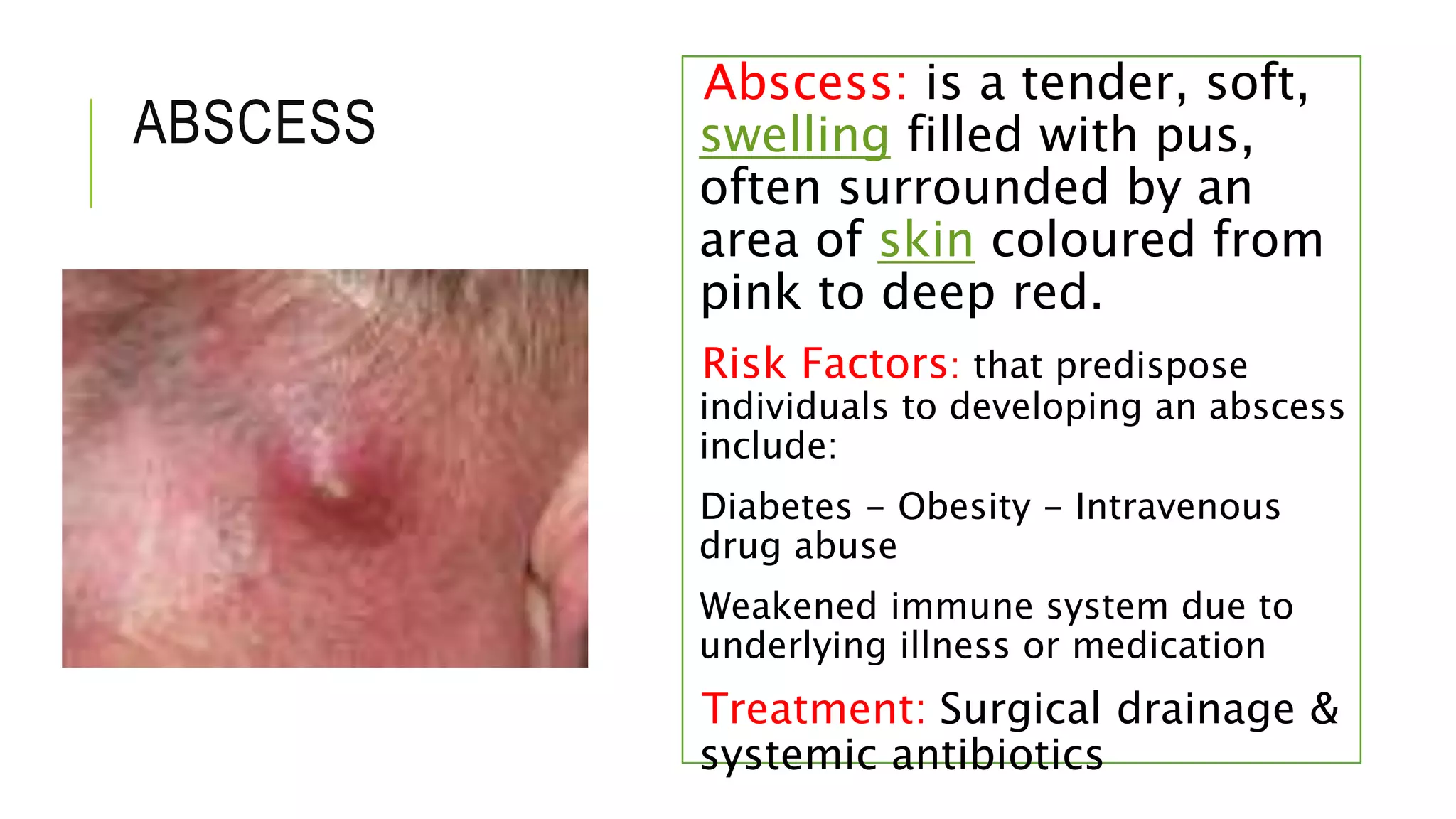
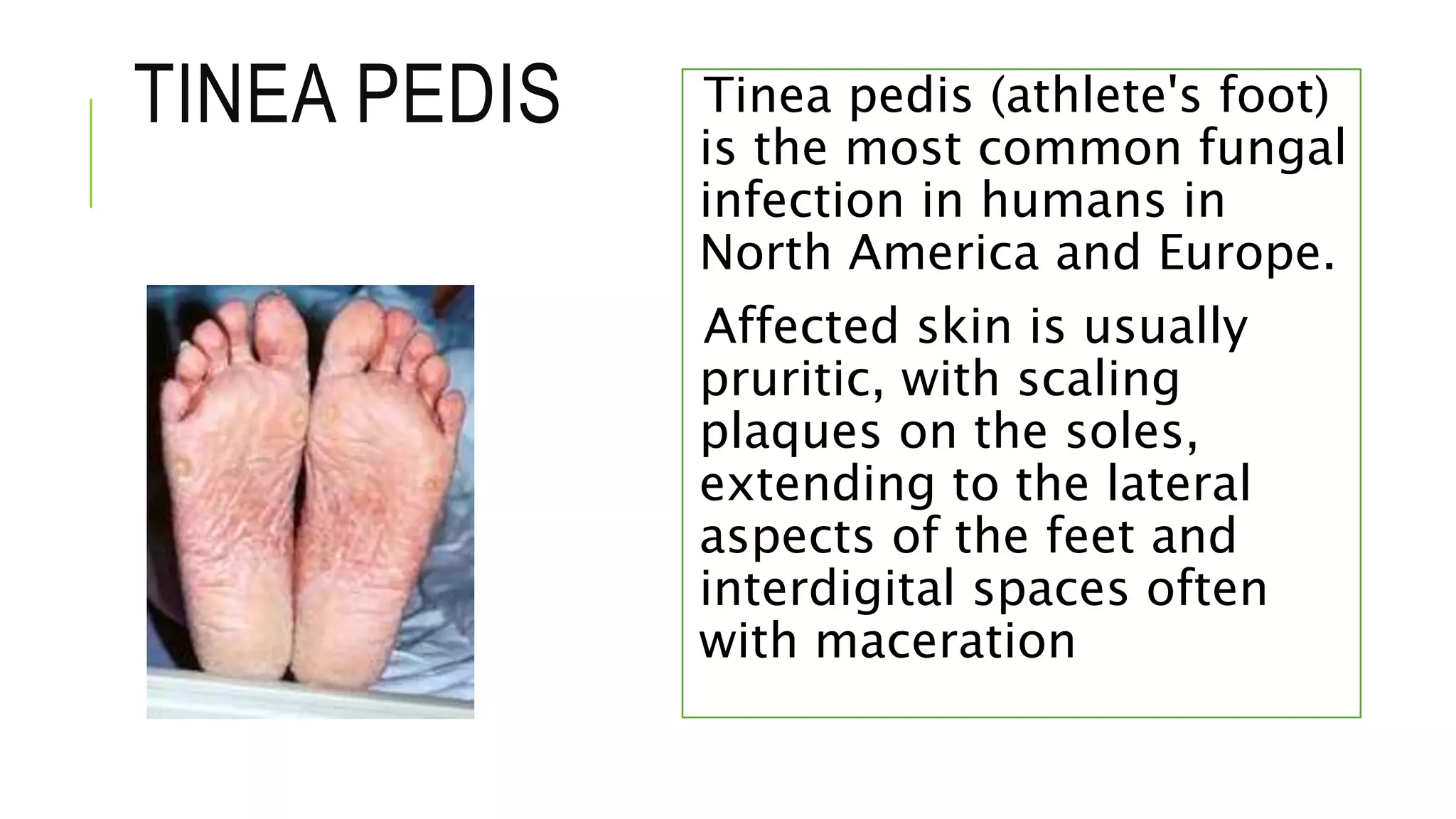
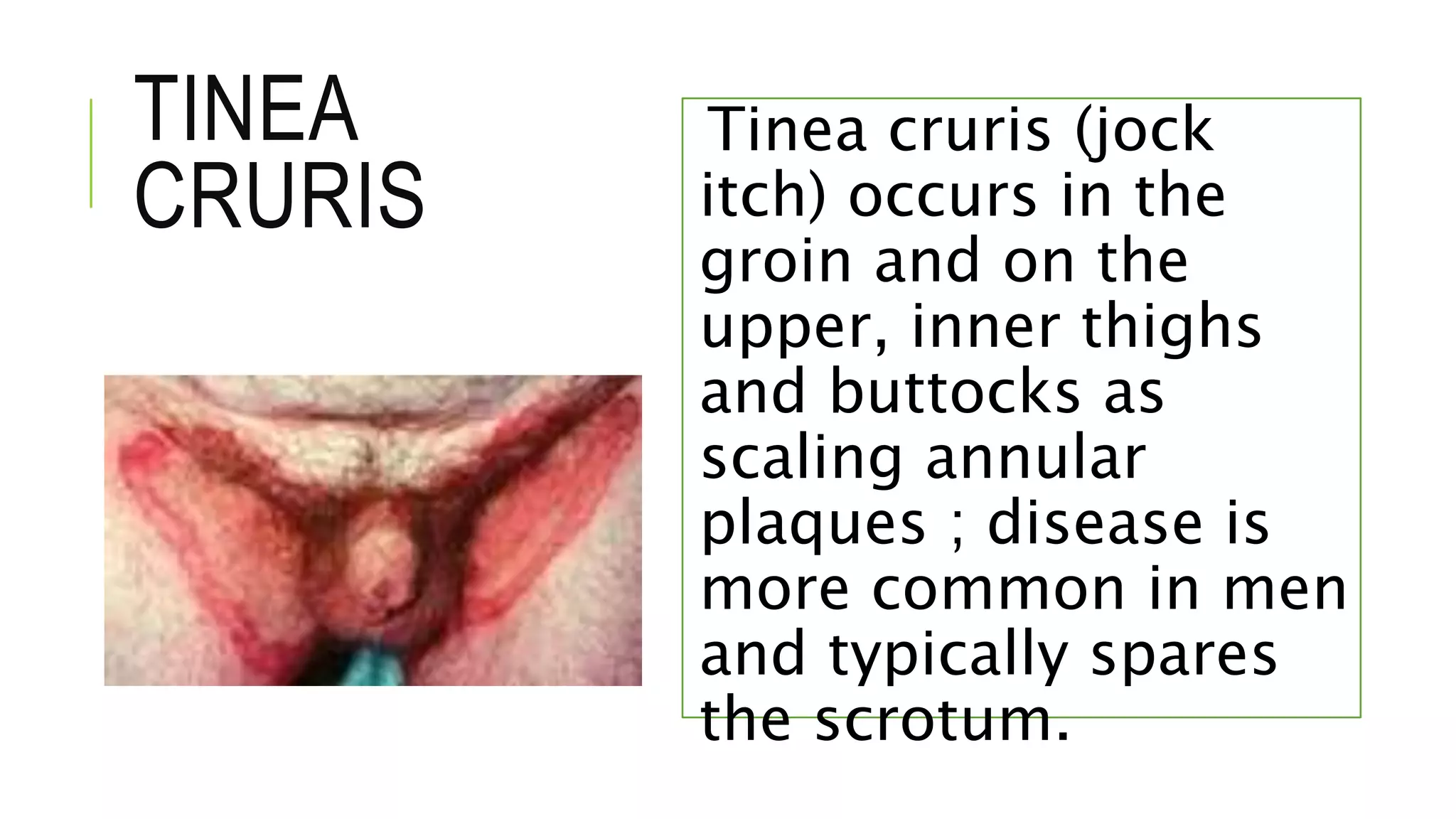
This document provides information on common skin infections, including their causes, presentations, and treatments. It discusses bacterial infections like impetigo, folliculitis, and cellulitis; viral infections like herpes, shingles, and warts; and fungal infections like ringworm and candidiasis. For each type of infection, the document describes typical signs and symptoms and recommends first-line treatment approaches, which generally involve topical or oral antibiotics, antivirals, or antifungals depending on the infecting pathogen.
















![1.1.1. bacterial infection of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-1-bacterialinfectionofskincompatibilitymode-130325014737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




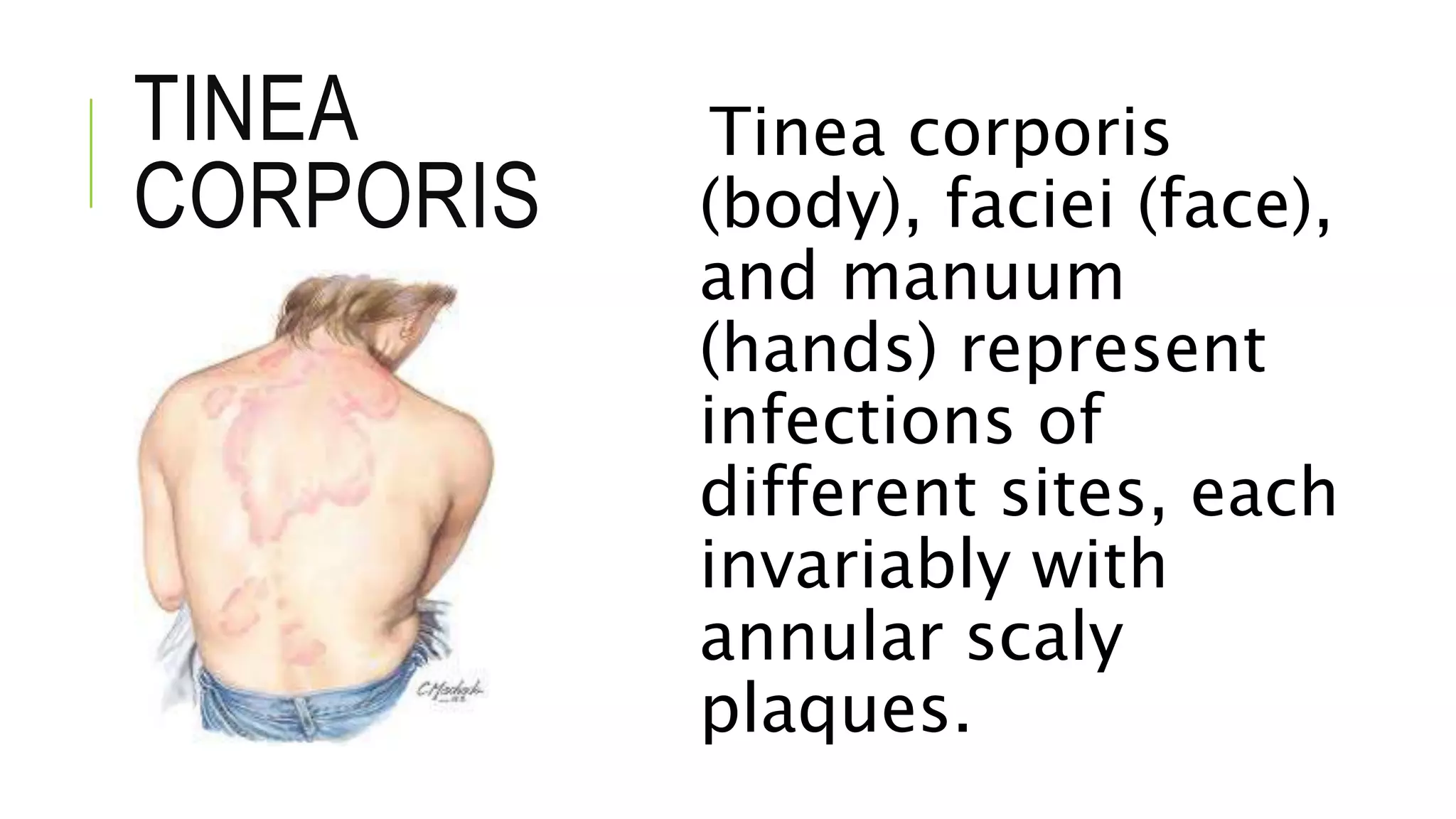
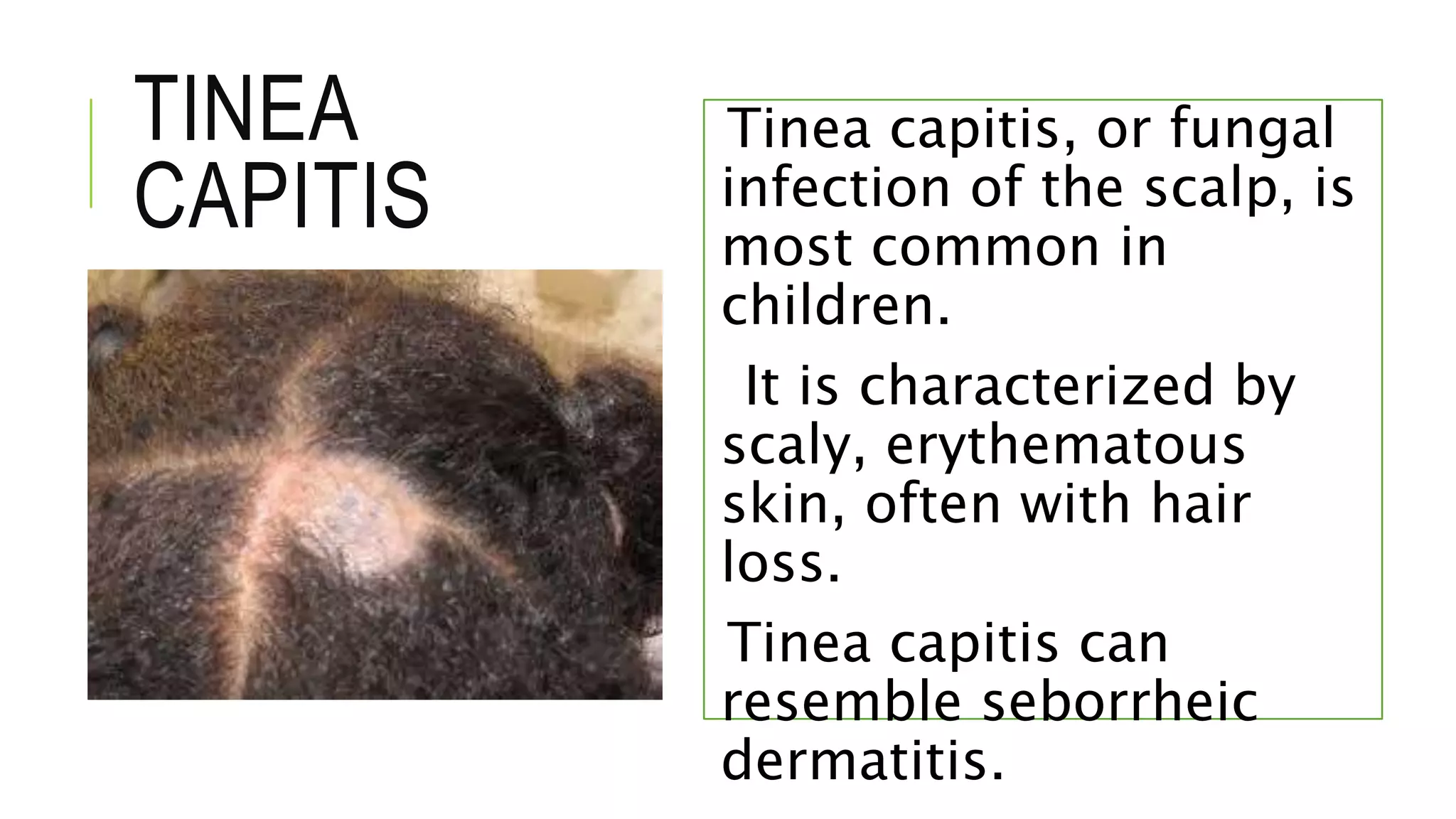
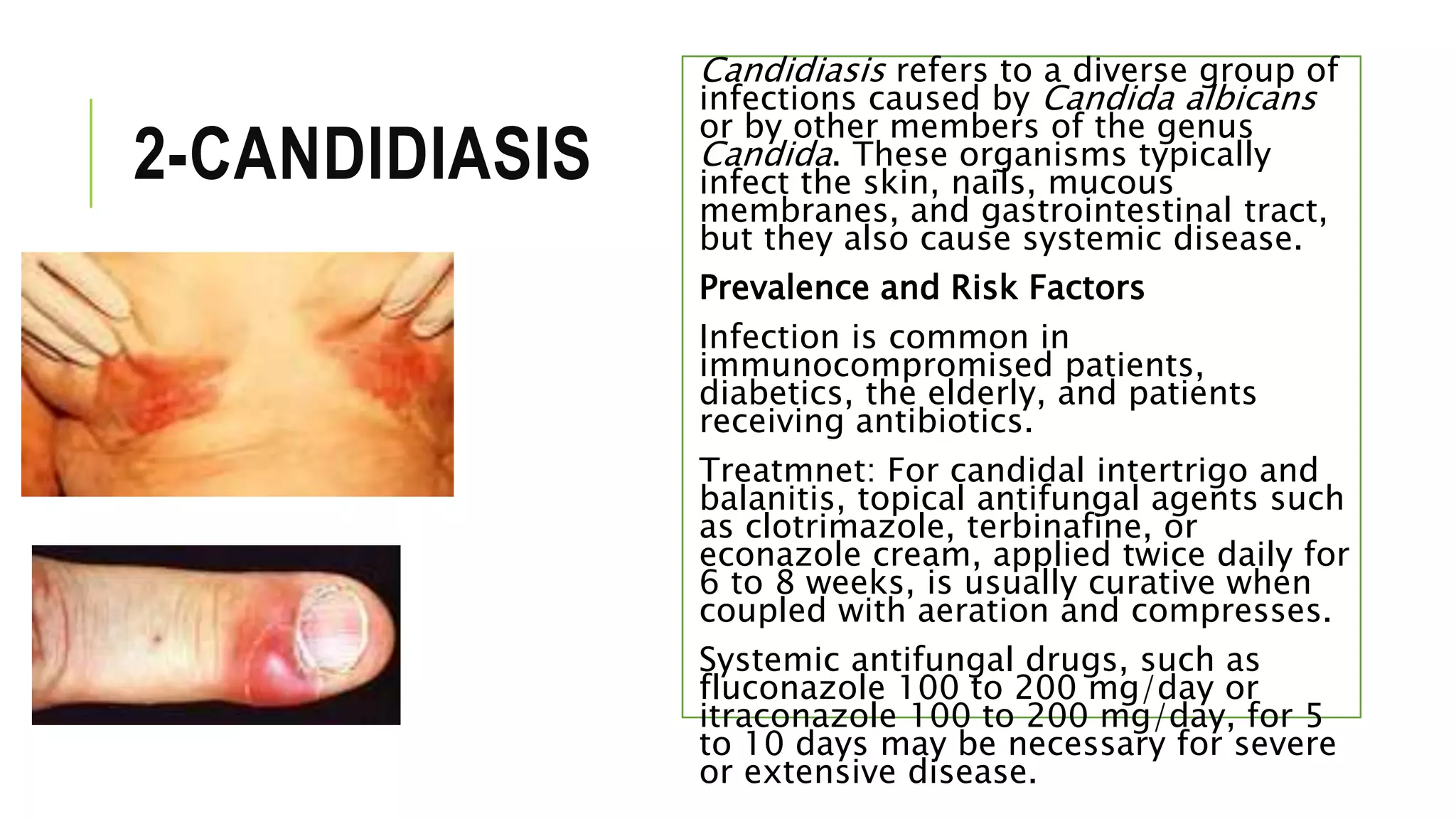
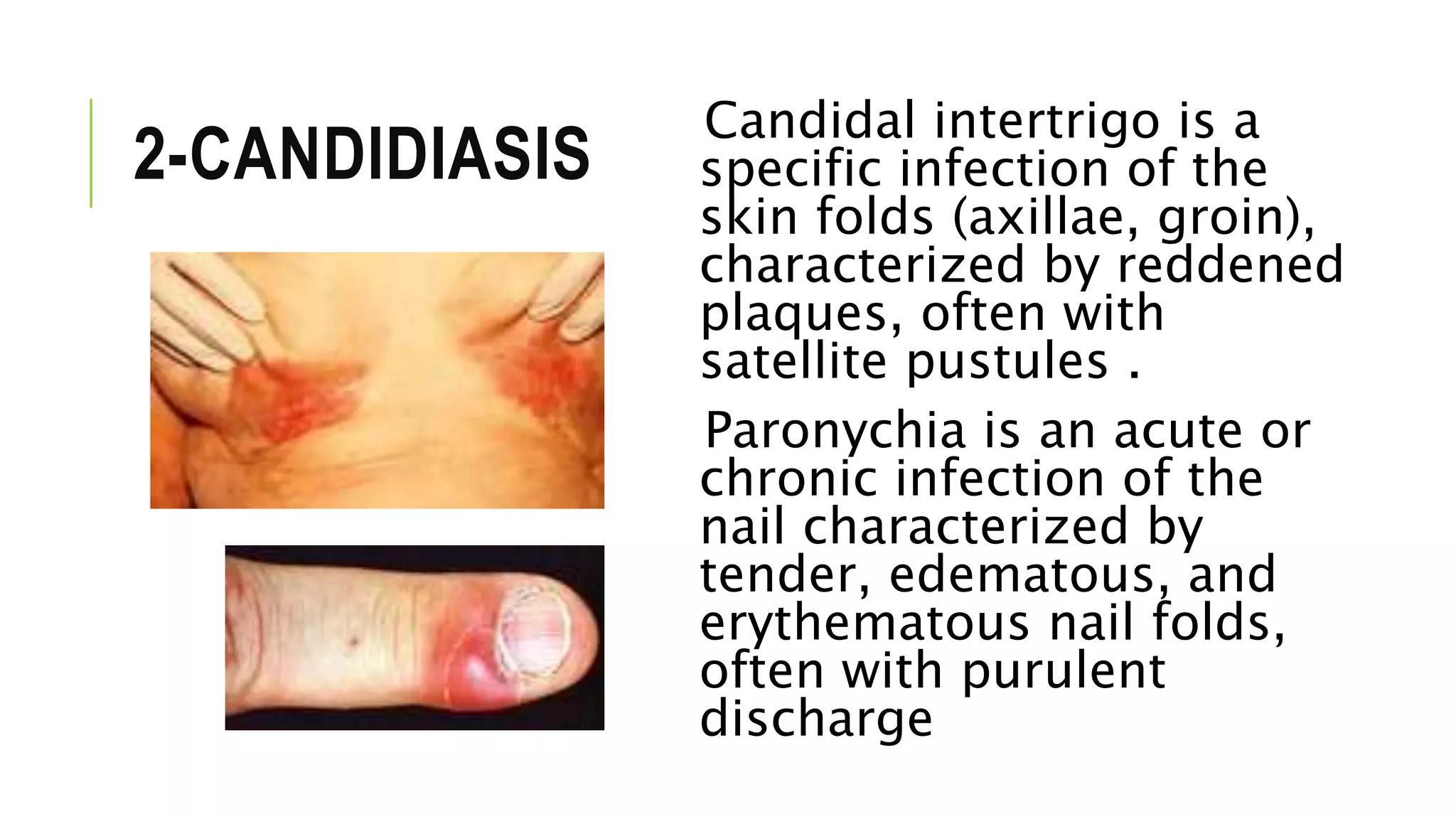
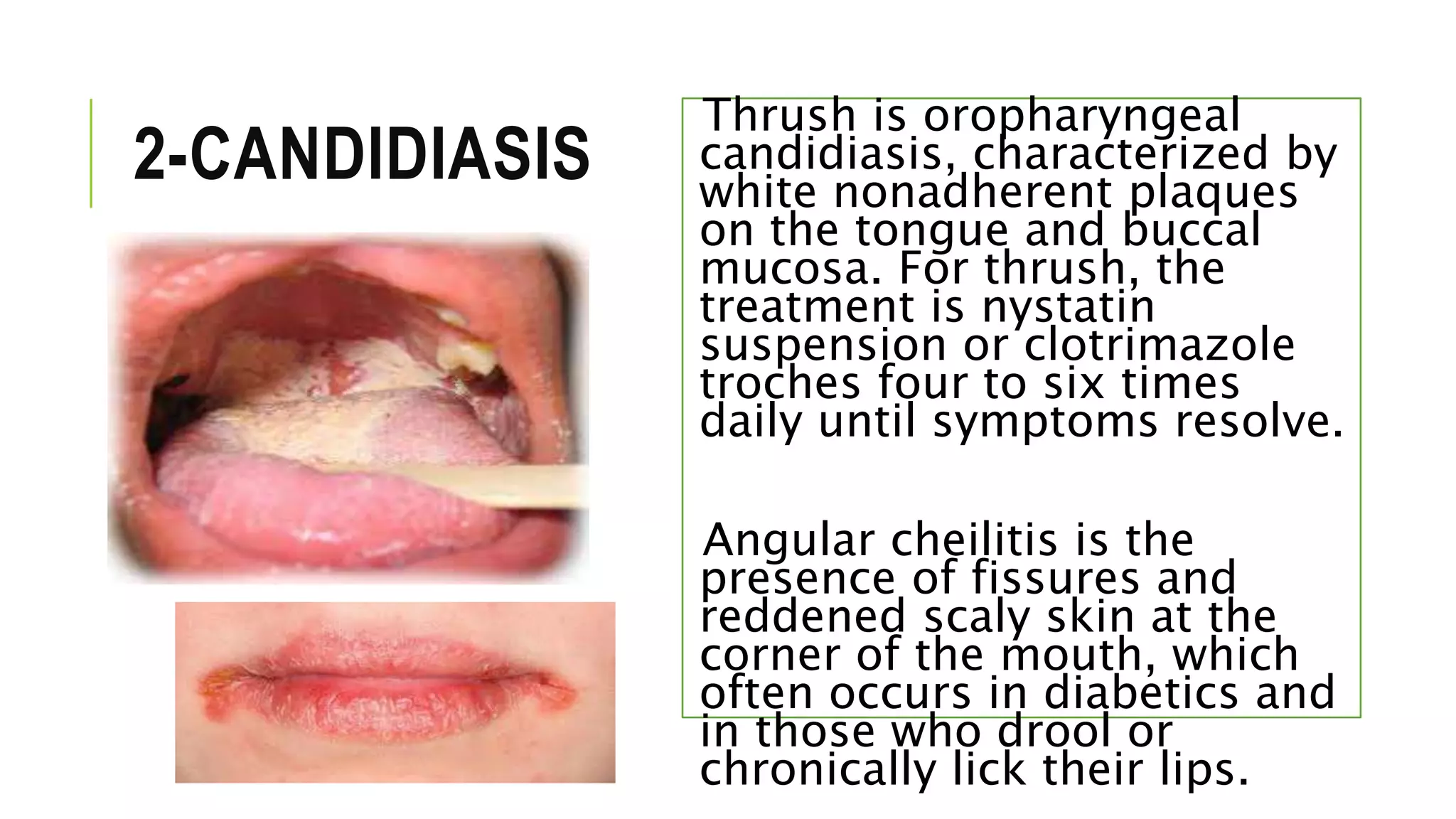
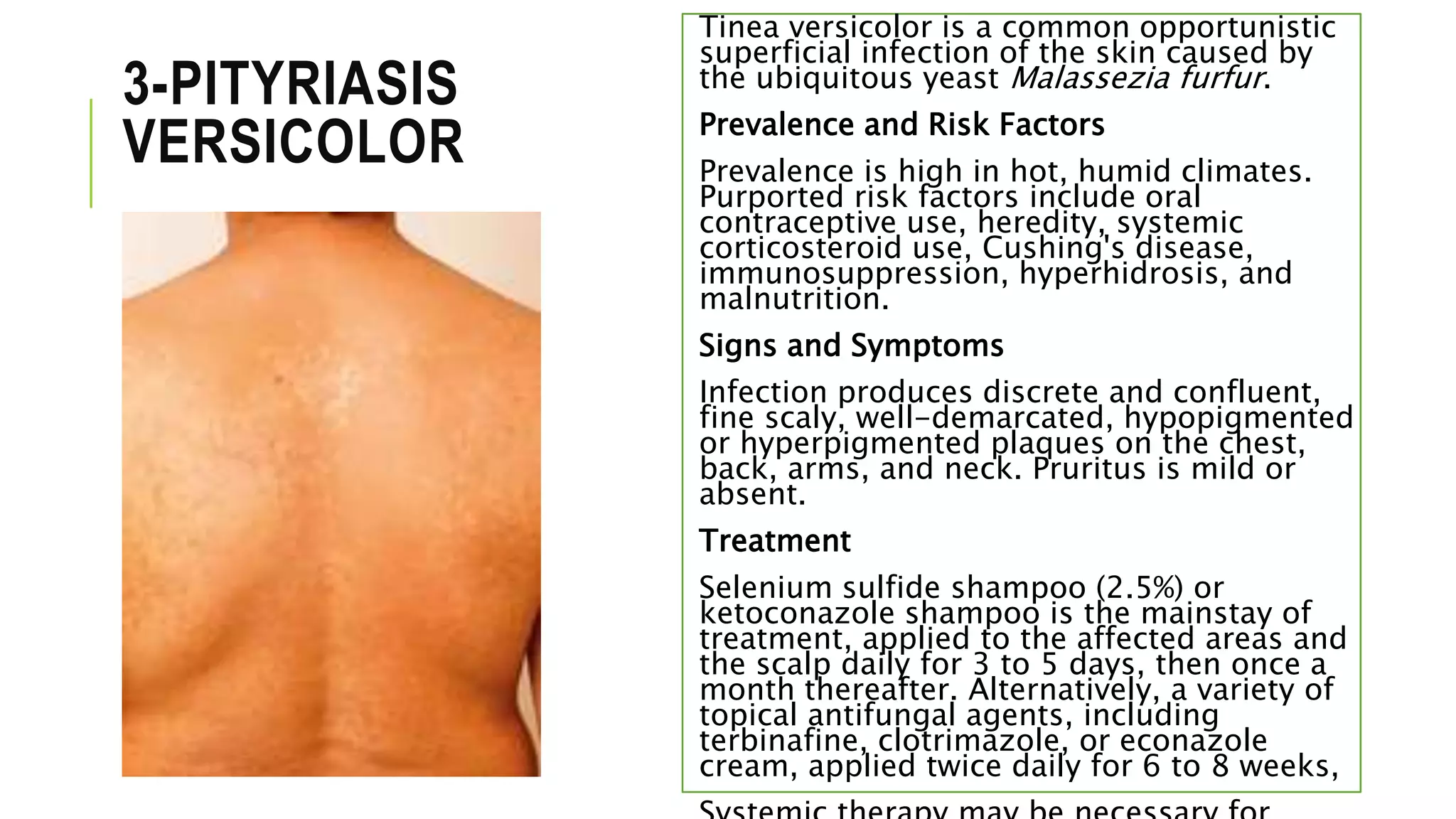
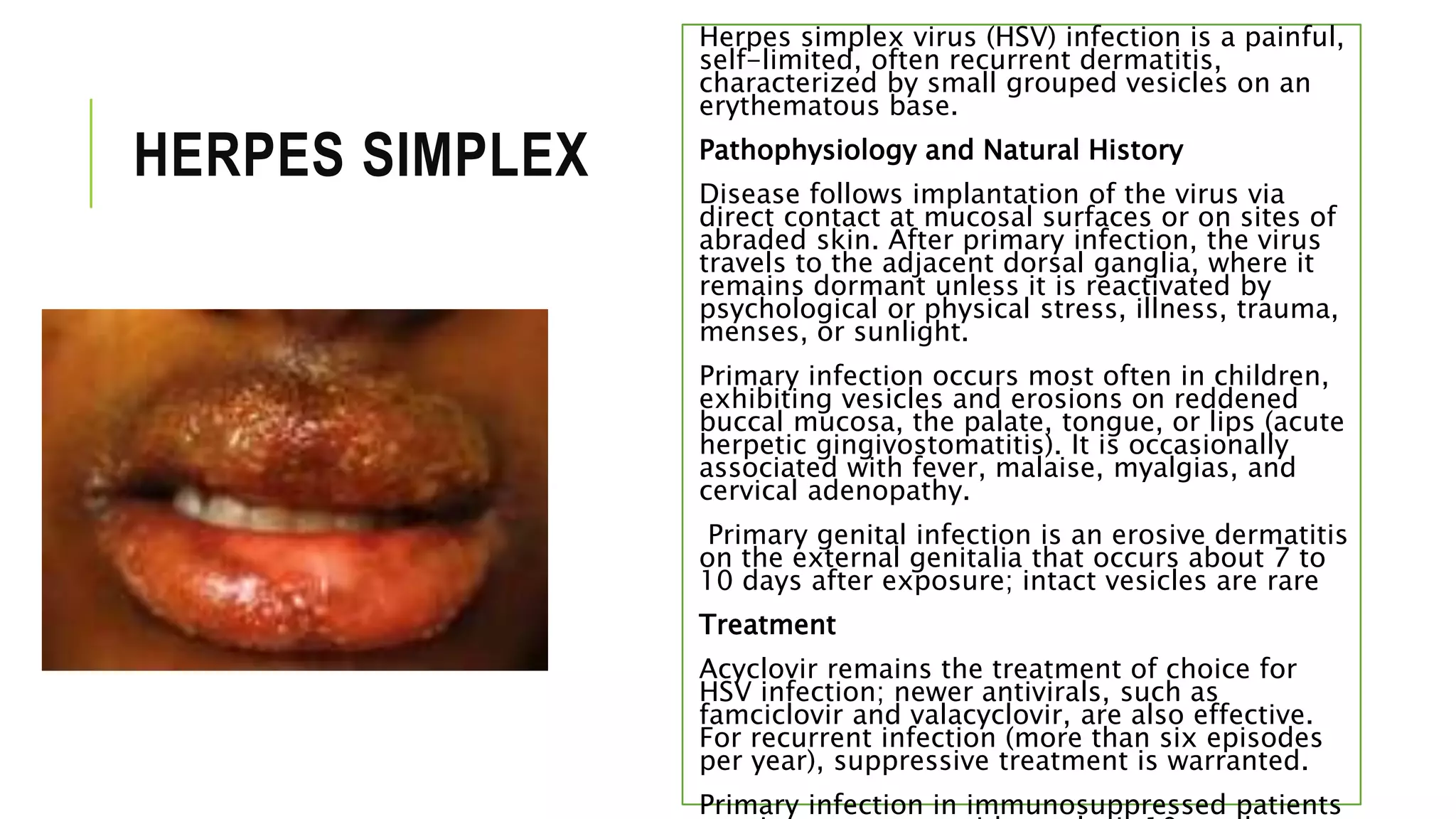
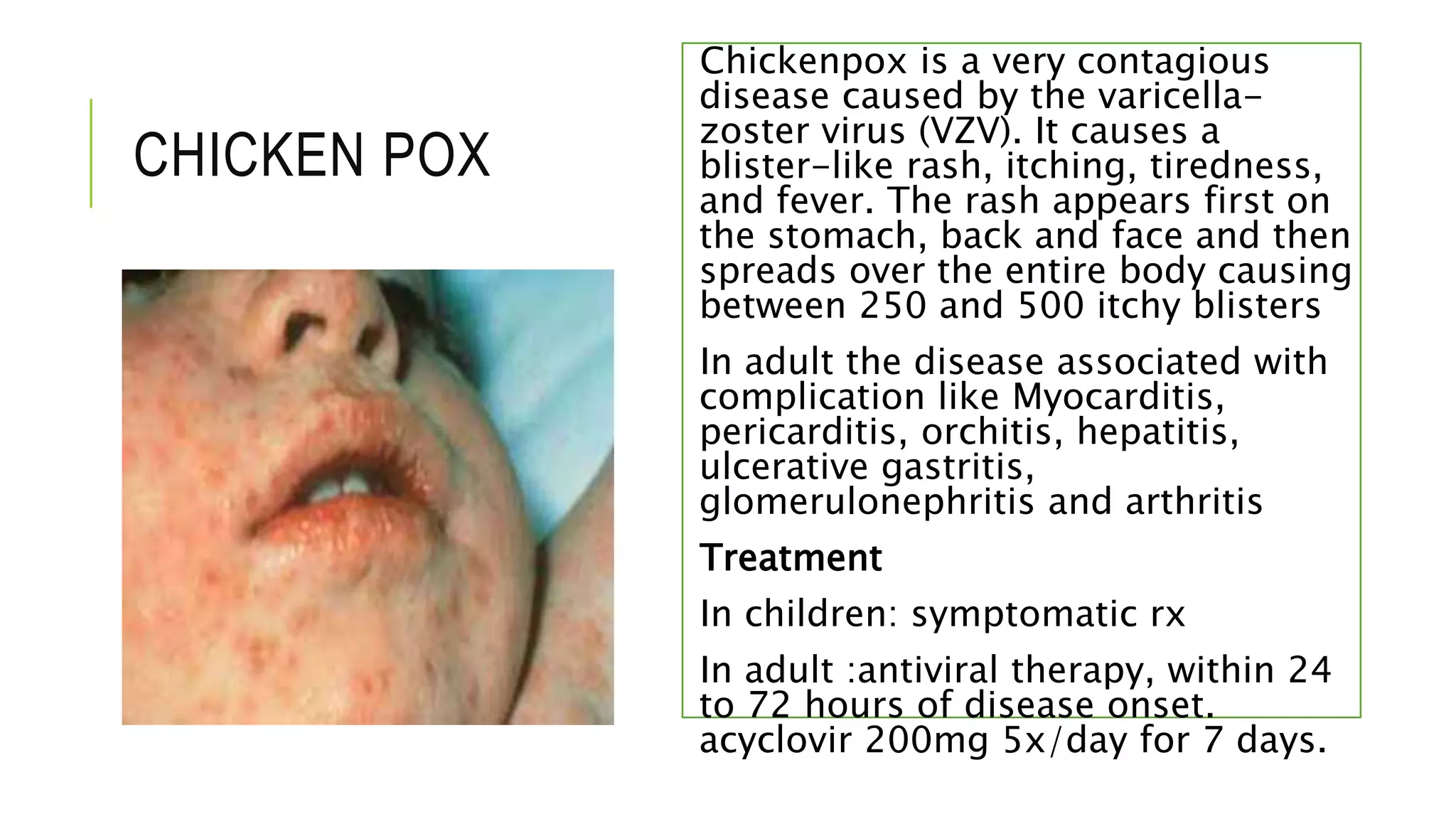
![Fungal infections of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/fungalinfectionsofskincompatibilitymode-130321223403-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
























































![Session 6 se and complications [repaired]](https://cdn.slidesharecdn.com/ss_thumbnails/session6seandcomplicationsrepaired-180404084057-thumbnail.jpg?width=640&height=640&fit=bounds)





















