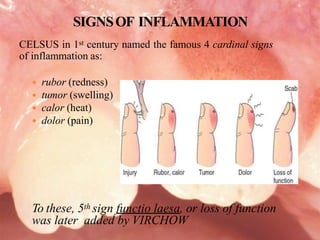
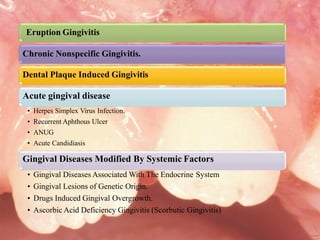
This document discusses various types of gingivitis and inflammation that can occur in children. It defines inflammation and lists its causes. The four classic signs of inflammation are redness, swelling, heat, and pain, with a fifth sign of loss of function added later. Acute inflammation comes on rapidly and is short-lived, while chronic inflammation has a gradual onset and longer duration. Specific types of gingivitis and inflammation discussed in children include eruption gingivitis, dental plaque-induced gingivitis, herpes simplex virus infection, acute necrotizing ulcerative gingivitis, acute candidiasis, chronic nonspecific gingivitis, and ascorbic acid deficiency ging