Download to read offline




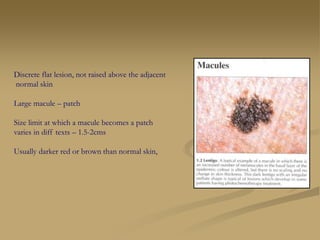

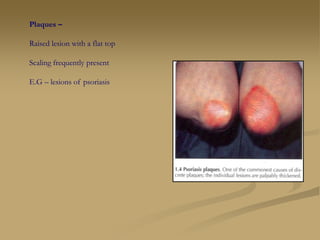

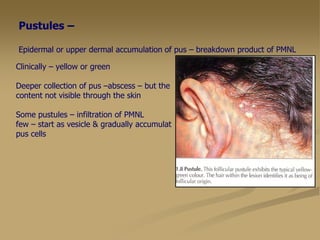
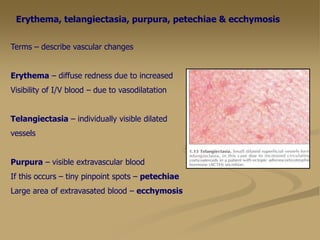



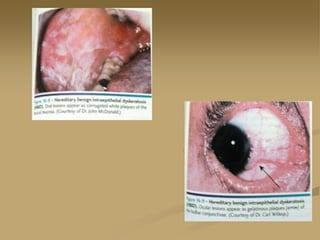
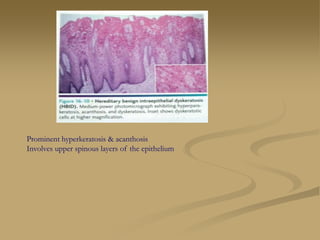






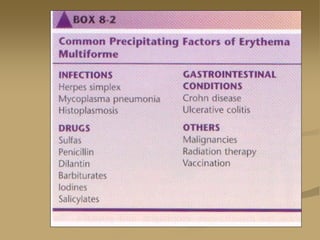
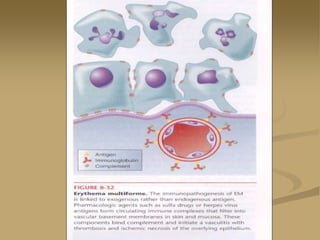

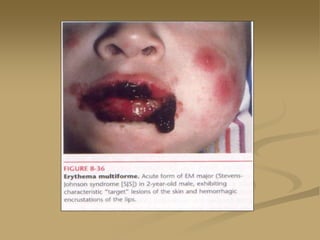
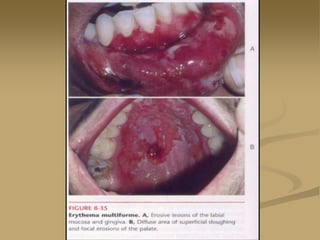
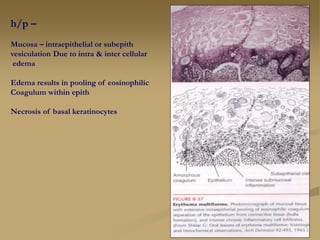
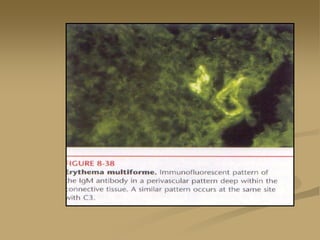
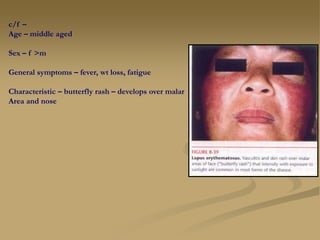
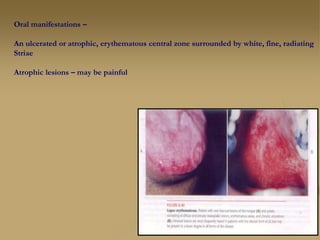







This document summarizes various skin diseases and their oral manifestations. It describes different skin lesions such as macules, papules, nodules, plaques, vesicles, bullae, pustules, and vascular changes. It then discusses specific diseases including ectodermal dysplasia, white sponge nevus, hereditary benign intraepithelial dyskeratosis, pemphigus, cicatrial pemphigoid, bullous pemphigoid, erythema multiforme, lupus erythematosus, and systemic sclerosis; and their oral signs and symptoms, histopathological features, and treatments.


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















