Downloaded 224 times
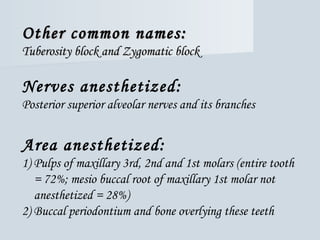
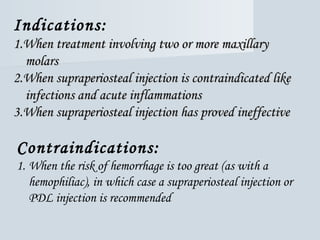
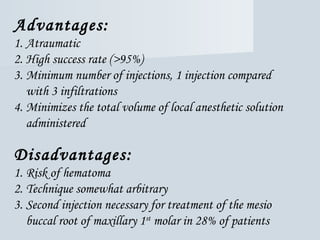
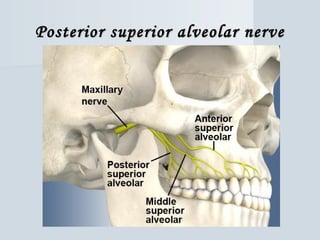
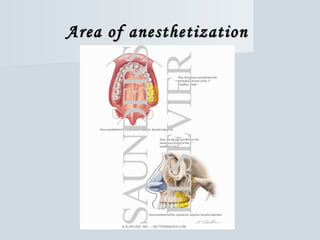
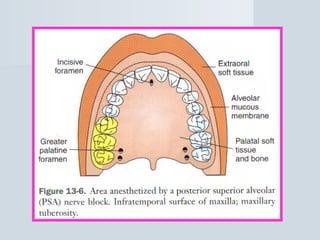

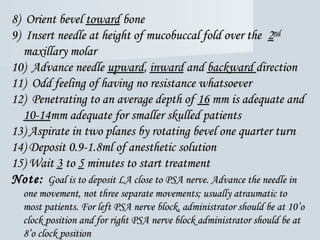



The posterior superior alveolar (PSA) nerve block is a widely used technique for anesthetizing the maxillary molars, though it may not sufficiently anesthetize the mesio buccal root of the maxillary first molar in up to 28% of patients. Key considerations include the risk of hematoma and the depth of needle penetration, with an average recommended depth of 16mm using a short needle. Indications for the PSA block include treatment of multiple maxillary molars and instances where supraperiosteal injection is contraindicated.





























![Techniques of local anesthesia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/techniquesoflocalanesthesiaautosaved-210618141111-thumbnail.jpg?width=640&height=640&fit=bounds)








































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



