Skin lesion morphology– Primary skin lesions
• Macule – circumscribed flat skin lesion – seen but not felt. Can be ill defined or well defined.
Hyperpigmented, hypopigmented or erythematous
• Papule – solid elevated lesion < 0.5 cm
• Vesicle – fluid filled lesion < 0.5 cm
• Nodule – solid elevated lesion > 0.5 cm
• Pustule – vesicle filled with pus
• Blister (bullae) – fluid filled lesion > 0.5 cm
• Plaque – A large > 1cm raised lesion, can be distinct or merging into the surrounding skin
• Wheal – dermal edema with papule or plaque
• Purpura and ecchymosis – erythematous macule with extravasation of blood - < 0.5cm –
purpura, > 0.5cm ecchymosis
• Lesions due to dilation of blood vessels – Telangectasia and poikiloderma (atrophy of skin,
telangiectasia and reticulate hyperpigmentation
4.
Papules and nodules– further morphology
• Vertical profile – dome shaped, flat topped, umbilicated, acuminate,
verrucous, pedunculated
• Horizontal profile – discoid, annular, circinate, arcuate, reticulate
Psoriasis
Describe the skinlesions
• Well defined, erythematous plaques with large silvery loose scales
• Initial lesions – discoid, gyrate, polycyclic and annular
• Positive auspitz sign
• Positive Koebner phenomenon
• Predilection – pressure points, scalp, nape of the neck, extensor
surfaces
13.
Describe the hands
•Well defined, erythematous plaques with large silvery loose scales
• Confluent plaques
• Nail changes – nail pitting, thickening of the nail plate, sub-ungual
hyperkeratosis, nail plate dystrophy, onycholysis, oil spots
15.
Describe the hands
Whatare the clinical types of articular involvement in psoriasis?
• Asymmetrical oligoarthritis
• Distal interphalangeal joint arthritis
• Symmetrical polyarthritis
• Arthritis mutilans
• Spondyloarthritis
What are thecommon precipitants of the disease?
• Physical trauma, infection – Streptococcal, HIV, drugs – antimalarials,
lithium, beta blockers, NSAIDs
What are the pathological hallmarks of the disease?
• Increased epidermal cell proliferation and parakeratosis, dermal
capillary and fibroblast proliferation
26.
What are theprinciples of therapy?
• Counselling and reassurance
• Topical agents – coal tar with salicylic acid, dithranol, calcipotriol,
steroids
• Systemic agents – MTX, acitretin
• Immunosupression – CyA
• Biologics
• Photochemotherapy – PUVA
• Herald patch– oval lesion wrinkled, salmon pink center and a
colarette of scales at the periphery
• Scaly papules arranged peripherally – fir tree appearance (Christmas
tree appearance)
• Trunk
• Diagnosis – Pityriasis rosea
32.
What is thepathogenesis of this condition?
• Viral agents implicated in the pathogenesis (HHV)
What are the principles of treatment?
• Is usually a self limiting condition
37.
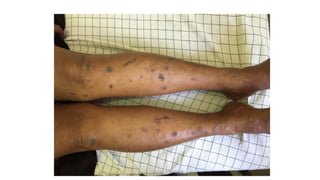
Describe the skinlesions
• (Pruritic), polygonal, purple (violaceous), plane papules
• Flexor aspect of the forearm and wrist
• Also shins
• Wickham’s striae on the lesions
• Oral lesions
38.
• Oral lesions– white, reticulate pattern in the oral mucosa, purplish
• Wickham’s striae
39.
• Scalp andnail lesions
• Nail – Thinning and splitting of the nail plate, longitudinal ridging,
pterygium formation
• Scalp demonstrates scarring alopecia
• Note – LP can also affect the mucosal surfaces
43.
What are theprinciples of therapy?
• Localized Lichen planus – topical steroids (medium potency)
• Extensive – oral steroids, acitretin
• Hypertropic LP – Potent topical steroids and salicylic acid with
antihistamines
• Nails – oral steroids
54.
Allergic contact dermatitis
•The typical features of eczema depend on the time course of the
disease
• Acute – erythematous and edematous plaques, ill defined and
surrounded by papules, vesicles, pustules and exudates with
subsequent crusting
• Chronic – lichenification – hyperpigmentation, skin thickening and
increased skin markings
How would youevaluate this patient?
• Patch test
What are the principles of management?
• Remove trigger
• Hydration and use of emollients
• Acute phase – Soaks of potassium permanganate as topical treatment, topical
steroids, rarely systemic steroids
• Chronic phase – Topical steroids, combined with salicylic acid/urea for
lichenified lesions
• Antibiotics for superadded infection
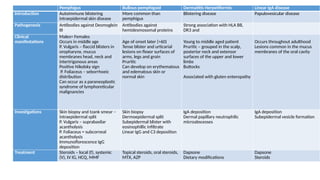
Pemphigus Bullous pemphigoidDermatitis Herpetiformis Linear IgA disease
Introduction Autoimmune blistering
intraepidermal skin disease
More common than
pemphigus
Blistering disease Papulovesicular disease
Pathogenesis Antibodies against Desmoglein
III
Antibodies against
hemidesmosomal proteins
Strong association with HLA B8,
DR3 and
Clinical
manifestations
Males= Females
Occurs in middle age
P. Vulgaris – flaccid blisters in
oropharynx, mucus
membranes head, neck and
intertrigonous areas
Positive Nikolsky sign
P. Foliaceus – seborrhoeic
distribution
Can occur as a paraneoplastic
syndrome of lymphoreticular
malignancies
Age of onset later (>60)
Tense blister and urticarial
lesions on flexor surfaces of
arms, legs and groin
Pruritic
Can develop on erythematous
and edematous skin or
normal skin
Young to middle aged patient
Pruritic – grouped in the scalp,
posterior neck and extensor
surfaces of the upper and lower
limbs
Buttocks
Associated with gluten enteropathy
Occurs throughout adulthood
Lesions common in the mucus
membranes of the oral cavity
Investigations Skin biopsy and tzank smear –
intraepidermal split
P. Vulgaris – suprabasilar
acantholysis
P. Foliaceus = subcorneal
acantholysis
Immunoflorescence IgG
deposition
Skin biopsy
Dermoepidermal split
Subepidermal blister with
eosinophillic infiltrate
Linear IgG and C3 deposition
IgA deposition
Dermal papillary neutrophilic
microabscesses
IgA deposition
Subepidermal vesicle formation
Treatment Steroids – local (f), systemic
(V), IV IG, HCQ, MMF
Topical steroids, oral steroids,
MTX, AZP
Dapsone
Dietary modifications
Dapsone
Steroids
68.
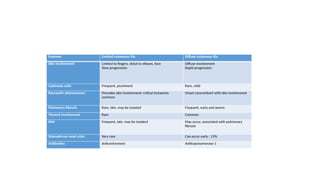
Features Limited cutaneousSSc Diffuse cutaneous SSc
Skin involvement Limited to fingers, distal to elbows, face
Slow progression
Diffuse involvement
Rapid progression
Calcinosis cutis Frequent, prominent Rare, mild
Raynaud’s phenomenon Precedes skin involvement: critical ischaemia
common
Onset concomitant with skin involvement
Pulmonary fibrosis Rare, late, may be isolated Frequent, early and severe
Visceral involvement Rare Common
PAH Frequent, late, may be isolated May occur, associated with pulmonary
fibrosis
Scleroderma renal crisis Very rare Can occur early ; 15%
Antibodies Anticentromere Antitopoisomerase-1
69.
What are theinvestigations you would like to perform in this patient?
• Skin biopsy – sclerosis of the dermis
• Serological – Anti centromere antibodies in LcSSC and Scl-70 in DSSC
• Other investigations for organ evaluation
What are the principles of management?
• General management for RP
• Nifedipine
• Treat esophageal reflux
• Immunosupression – steroids, MTX, AZA
• D- penicilamine in diffuse disease
71.
PRP
• Plaques withcoalescing follicular scaly papules
• Orange colored thickening of the palms
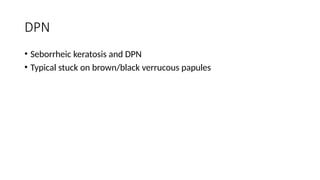
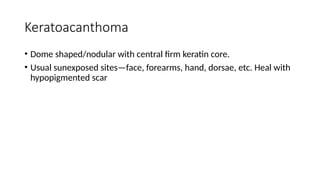
Keratoacanthoma
• Dome shaped/nodularwith central firm keratin core.
• Usual sunexposed sites—face, forearms, hand, dorsae, etc. Heal with
hypopigmented scar
Melanoma Basal cellcarcinoma Squamous cell carcinoma
Introduction Skin malignancy arising from melanocytes Arises from undifferentiated epidermal cells Malignant proliferation of keratinocytes
Pathogenesis and epidemiology Incidence increasing
Risk factors
Exposure to UV radiation
Family history
Multiple pigmented melanocytic naevi, giant
melanocytic naevi
Severe burns in childhood
Common in Europe
Risk factors
Exposure to UV radiation
Arsenic, immunosupression
Genetic predisposition – Xeroderma
pigementosum
Risk factors
Exposure to UV
Arsenic, immunosupression
From long standing ulcers
From existing lesions – Bowen’s disease
(intraepidermal lesion confined to hair follicle, actinic
keratosis
Clinical manifestations Sites – over the back (males) and lower limbs
(females)
Change in a melanocytic naevus
Increase in size (>6mm), irregular outline,
asymmetry, alteration of colour, bleeding and
ulceration, satellite lesions, change in
symptoms
Subtypes
Superficial spreading – flat/nodular lesions
Lentigo melanoma – face of elderly patients
Acral melanoma – hands and feet
Amelanocytic melanoma
Sun exposed areas of the face – especially the
nose
Subtypes
Nodulocystic – dome shaped, pearl colour with
superficial telengectasia, central ulceration and
rolled edges
Superficial – plaque like lesion commonly in the
trunk
Sclerosing – late presentation
Pigmented
Metastasis rare – local destruction common
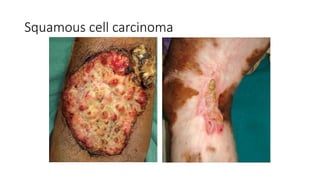
Indurated nodule or ulcer in sun exposed areas
Local infiltration, lymphatic metastasis
Investigations Skin biopsy and sentinel node biopsy Skin biopsy Skin biopsy
Management Prognosis depends on depth of invasion –
Breslow thickness
Surgical resection
Chemotherapy, alpha interferron for
metastatic melanoma -
Resection for high risk lesions – facial, sclerosing
Cryotherapy, radiotherapy, PDT, imiquomod -
immunotherapy
Surgical resection, radiotherapy