Downloaded 263 times


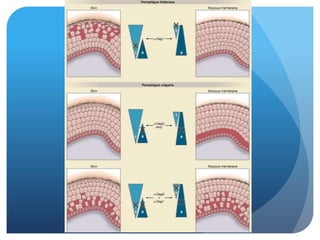
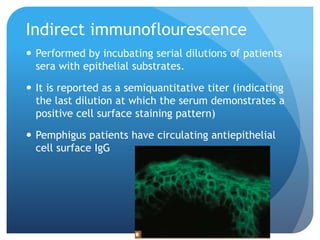
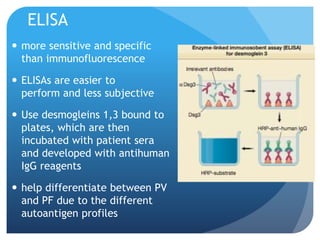

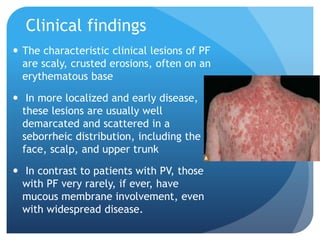




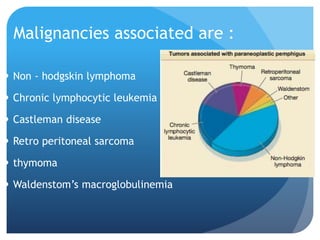
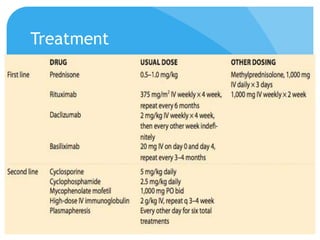

This document summarizes several intra-epidermal blistering disorders including pemphigus vulgaris, pemphigus foliaceus, and paraneoplastic pemphigus. Pemphigus vulgaris is characterized by suprabasal acantholysis and antibodies against desmoglein 3. Pemphigus foliaceus involves subcorneal acantholysis and antibodies against desmoglein 1. Paraneoplastic pemphigus is associated with an underlying neoplasm and antibodies against both desmogleins and plakins. Treatment for these disorders involves high dose corticosteroids along with immunosuppressive agents.
















































![[Chronic Multiple ulcers] O.Medicine lab](https://cdn.slidesharecdn.com/ss_thumbnails/o-250128123323-29e53ff5-thumbnail.jpg?width=640&height=640&fit=bounds)
























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
