The document discusses the principles of color theory, specifically as it relates to shade selection in dentistry. It covers various color systems, influences on color perception, and the importance of understanding factors like hue, chroma, value, and translucency for effective shade matching. The knowledge of these aspects is essential for dental practitioners to achieve natural-looking restorations.

















![Shade Selection
Page: 22 of 40
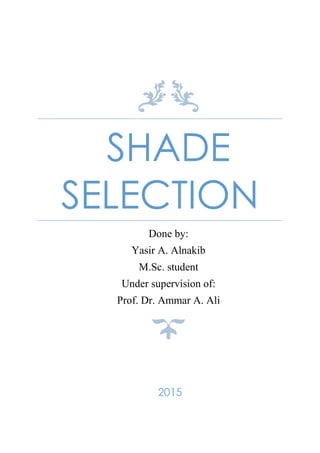
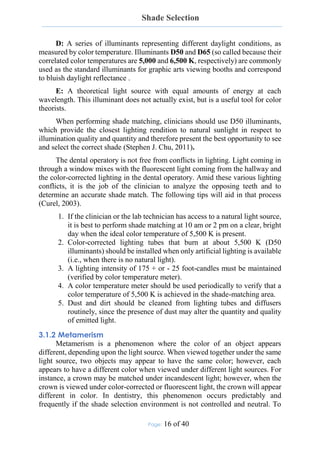
When illuminated, opals and enamel will trans-illuminate the reds and
scatter the blues within its body. This is why enamel appears bluish at the incisal
edge even though it is colorless (Fig. 19 c ) (Bosch, et al., 1995). The opalescent
effects of enamel brighten the tooth and give it optical depth and vitality (Garber,
2000)
.
Figure 19 In vitro examples of light effects exhibited by a natural tooth. Natural
light effects (a), fluorescence (b), opalescence (blue [c] and orange [d])
3.6 REFLECTIONS OF LIGHT
It is important to realize that matching the hue and chroma is sixth or
seventh in importance on the list of things to match when constructing a prosthetic
replacement. You have to be fairly close to someone to detect subtle differences
in hue; yet shape, value, surface texture, luster, and opacity disparities can be seen
from four or five feet away or more. Violating conformity of the unique
characteristics of the natural dentition will cause an unwanted prominence of your
restoration. (Glick, 1994)
These characteristics determine how light is reflected, transmitted, or
scattered thus affecting its hue, chroma, value, and translucency. The appearance
of teeth is mostly determined by how light interacts with the curved and varied
surface. (Glick, 1994)
3.6.1 Surface Texture
A roughened surface texture will not yield as well defined an image and
will scatter the light and the individual wavelengths will all bend differently
yielding a substantially different spectrum returning to the eye. (Obregon, 1981)
Texture can be broken down into subgroups: vertical, horizontal, and
malformations. Vertical surface textures are primarily composed of the heights of
contour of the marginal ridges and the developmental lobes. Perichymata, the
fine transverse wavelike grooves believed to be external manifestations of the
striae of retzius are horizontal textures. The striae or lines of retzius are the result
of the layering manner in which the deposition of enamel takes place.
Malformations are the third textural group and can be from cracks, chips, and
other surface aberrations (Fondriest, 2003).](https://image.slidesharecdn.com/shadeselection-150724155751-lva1-app6891/85/Shade-selection-23-320.jpg)





![Shade Selection
Page: 28 of 40
4.1.3.1 Steps of Using the Vita 3D-Master
The first step in using the Vita 3D-Master system is to make sure the tabs
are aligned vertically. Misaligned tabs can be distracting to the operator. The
patient is asked to smile then the Toothguide Vita 3D-Master is used in 3 steps
as follows:
1. Value determination: Shade guide is passed adjacent to the teeth,
going from the darker shades through the intermediate to the lighter
shades. The user selects the value level (from 0 to 5, with 0 being the
lightest [high value] and 5 being the darkest [low value]) that is
closest to the value of the tooth to be matched, and then takes the
medium (M) shade sample from the selected value group
2. Chroma determination: The user selects the color sample from the
M group with the chroma level (from 1 to 3, with 1 being the least
chromatic and 3 being the most chromatic) that is closest to that of
the tooth to be matched.
3. Hue determination: shade than the color sample of the M group
selected in the second step. Now the best-matching shade sample can
be determined and the information recorded in the color
communication form.
Several readings are necessary to create a color map of a tooth. Typically at
least three readings per tooth are suggested, one each for the gingival, middle,
and incisal thirds.
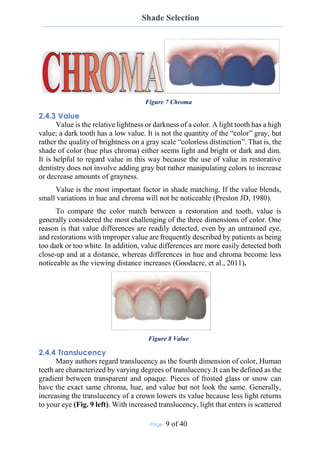
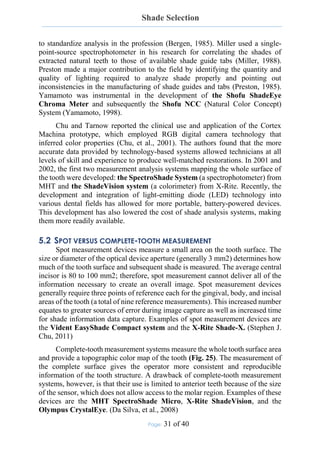
The Linearguide Vita 3D-Master (Fig. 24) has the same shade tabs as the
Toothguide but a different design, and shade matching is reduced to two steps:
1. Value selection: A dark-gray holder, containing only 6 middle tabs
(0M2 to 5M2) is used. The small number of tabs with large color
differences and the linear tab arrangement simplify group selection.
2. Chroma and hue selection: A final selection based on chroma and hue
is made from the initial value group selected.
Figure 24 Linearguide VITA 3D-Master shade guide system](https://image.slidesharecdn.com/shadeselection-150724155751-lva1-app6891/85/Shade-selection-29-320.jpg)








![Shade Selection
Page: 38 of 40
6 REFERENCES
1. AH.Munsell A grammar of color [Book]. - NY : Van Nostrand Reinhold,
1969.
2. Aschheim Kenneth W. Esthetic Dentistry - A Clinical Approach to
Techniques and Materials [Book]. - [s.l.] : Mosby, 2015. - Vol. 3.
3. Avery D. New shade-matching technology: The final piece of the shade
communication puzzle [Journal]. - [s.l.] : J Dent Technol , 2003. - 6 : Vol.
20.
4. Bergen SF. Color in aesthetics. [Journal]. - [s.l.] : N Y State Dent J, 1985. -
Vol. 51.
5. Bosch J. and Coops JC. Tooth color and reflectance as related to light
scattering and enamel hardness. [Journal]. - [s.l.] : J. Dent. Res, 1995. - 1 :
Vol. 74.
6. Brewer JD,, Wee A and R. Seghi Advances in color matching. [Journal]. -
[s.l.] : Dent Clin North Am, 2004. - Vol. 48.
7. Carsten Successful shade matching—What does it take? [Journal]. - [s.l.] :
Compend Contin Educ Dent, 2003. - Vol. 24. - pp. 175–178.
8. Chu SJ. and DP. Tarnow Digital shade analysis and verification: A case
report and discussion [Journal]. - [s.l.] : Pract Periodontics Aesthet Dent,
2001. - Vol. 13.
9. Cornell D. and Winter R. Manipulating light with the refractive index of
an all-ceramic material [Journal]. - [s.l.] : Prac. Proced. Aesthet. Dent,
1999. - 1 : Vol. 8. - pp. 913-917.
10. CP. Sim, AU. Yap and J. Teo Color perception among different dental
personnel. [Journal]. - [s.l.] : Oper Dent, 2001. - Vol. 26. - pp. 435–439.
11. Curel Galip The Science and Art of Porcelain Laminate Veneers [Book]. -
[s.l.] : quintessence, 2003. - Vol. First edition.
12. Da Silva JD, [et al.] Clinical performance of a newly developed
spectrophotometric system on tooth color reproduction [Journal]. - [s.l.] : J
Prosthet Dent , 2008. - Vol. 99.
13. Fondriest james S. Shade matching in restorative dentistry: the science and
strategies. [Journal]. - [s.l.] : Int J Periodontics Restorative Dent, 2003. - 5 :
Vol. 23.
14. Freedman G. Communicating color [Journal]. - [s.l.] : Dent Today, 2001. -
Vol. 20.](https://image.slidesharecdn.com/shadeselection-150724155751-lva1-app6891/85/Shade-selection-39-320.jpg)
![Shade Selection
Page: 39 of 40
15. Freedman George CONTEMPORARY ESTHETIC DENTISTRY
[Book]. - St. Louis, Missouri : mosby, 2012. - Vol. first edition.
16. Garber D. The Quest for the All-Ceramic Restoration. [Journal]. - [s.l.] :
Quintessence Dental Technology, 2000.
17. Geller W Polishing porcelain makes a crown smoother, more translucent,
and improves the color [Journal]. - [s.l.] : QDT, 1983. - 6 : Vol. 7.
18. Glick K. Color and Shade Selection in Cosmetic Dentistry: Part III
Establishing the Proper Environment and Technique [Journal]. - [s.l.] : J. of
AACD, 1994. - Vol. summer.
19. Goodacre Charles J. and Sagel Paul A. Dental Esthetics in Practice: Part
3 - Understanding Color & Shade Selection. - [s.l.] : dentalcare.com
Continuing Education Course, 2011.
20. Goodkind RJ and Schwabacher WB. Use of fiber-optic colorimeter for in
vivo color measurement of 2830 anterior teeth [Journal]. - [s.l.] : J Prosthet
Dent , 1987. - Vol. 58.
21. Goodkind RJ., K. Keenan and WB. Schwabacher A comparison of
Chromascan and spectophotometric measurements of 100 natural teeth.
[Journal]. - [s.l.] : J Prosth Dent , 1985. - Vol. 53.
22. Ishigawa-Nagai S, Sato RR, Shiraishi A, Ishibashi K. Using a computer
color-matching system in color reproduction of porcelain restorations. Part
3: a newly developed spectrophotometer designed for clinical application.
[Journal]. - [s.l.] : Int J Prosthodont , 1994. - Vol. 7.
23. Ishikawa-Nagai S. [et al.] Using a computer color-matching system in
color reproduction of porcelain restorations. Part 1: Application of CCM to
the opaque layer [Journal]. - [s.l.] : Int J Prosthodont, 1992. - Vol. 5.
24. JADA. Dental Shade Guides. [Journal]. - [s.l.] : J Am Dent Assoc, 2002. -
133.
25. Judeh A. and " A. Al-Wahadni. A comparison between conventional
visual and spectrophotometric methods for shade selection [Journal]. -
[s.l.] : Quintessence international, 2009. - 9 : Vol. 40.
26. McLaren E. Luminescent Veneers [Journal]. - [s.l.] : J.Esthetic Dent,
1997. - 1 : Vol. 9.
27. Miller LL. A scientific approach to shade matching. In: Preston JD (ed).
Perspectives in Dental Ceramics: Proceedings of the Fourth International
Symposium on Ceramics. [Journal]. - [s.l.] : Quintessence, 1988.](https://image.slidesharecdn.com/shadeselection-150724155751-lva1-app6891/85/Shade-selection-40-320.jpg)
![Shade Selection
Page: 40 of 40
28. Obregon A. Effects of opaque and porcelain surface texture on the color of
ceramometal restorations [Journal]. - [s.l.] : J. Prosth. Dent., 1981. - 3 : Vol.
46.
29. Ontiveros JC and Paravina RD. Color change of vital teeth exposed to
bleaching performed with and without supplementary light. [Journal]. -
[s.l.] : J Dent, 2009. - Vol. 37.
30. Özat, Tuncel İ. and Eroğlu E. Repeatability and reliability of human eye
in visual shade selection [Journal]. - [s.l.] : Journal of Oral Rehabilitation,
2013. - Vol. 40.
31. Paravina RD. Performance assessment of dental shade guides. [Journal]. -
[s.l.] : J Dent , 2009. - Vol. 37.
32. Paravina RD., Powers JM. and Fay RM. Dental color standards: shade
tab arrangement. [Journal]. - [s.l.] : J Esthet Restor Dent , 2001. - Vol. 13.
33. Paul S [et al.] Visual and spectrophotometric shade analysis of human teeth
[Journal]. - [s.l.] : J Dent Res, 2002. - Vol. 81.
34. Preston JD Bergen SF Color science and dental art: a self-teaching
program, [Book]. - St Louis : mosby, 1980.
35. Preston JD. Current status of shade selection and color matching.
[Journal]. - [s.l.] : Quintessence Int, 1985. - Vol. 16.
36. R.Waltke Color in the human dentition [Book]. - NY : Jelenko, 1977.
37. Seungyee Kim, Brewer Jane D. and Davis Elaine L. Reliability and
accuracy of four dental shade-matching devices [Journal]. - [s.l.] : The
Journal of Prosthetic Dentistry, 2009. - 3 : Vol. 101.
38. Sproull RC. Color matching in dentistry, part I. The three-dimensional
nature of color. [Journal]. - [s.l.] : J Prosthet Dent, 1973. - Vol. 29.
39. Stephen J. Chu DMD, MSD, CDT, MDT, Alessandro Devigus, Dr MED
DENT, Rade D. Paravina, DDS, MS, PhD, Adam J. Mieleszko, CDT
Fundamentals of color : shade matching and communication in esthetic
dentistry [Book]. - [s.l.] : Quintessence Pub, 2011. - Vol. 2nd edition.
40. Sundar V. and Amber PL. Opals in nature. [Journal]. - [s.l.] : J. of Dental
Technology, 1999. - 8 : Vol. 16.
41. Yamamoto M. Development of the vintage halo computer color search
system. [Journal]. - [s.l.] : Quintessence Dent Technol, 1998. - Vol. 21.](https://image.slidesharecdn.com/shadeselection-150724155751-lva1-app6891/85/Shade-selection-41-320.jpg)

















































































