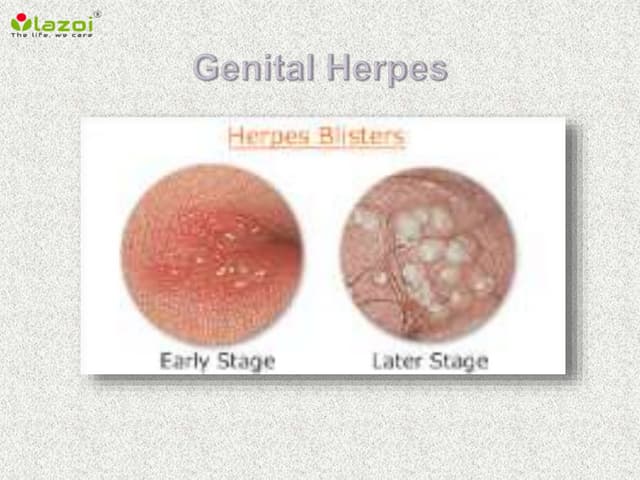
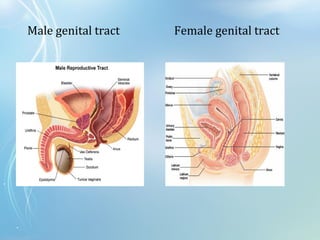

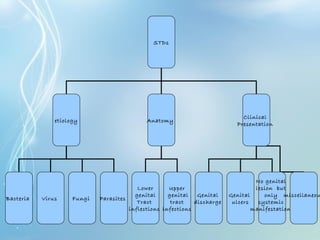
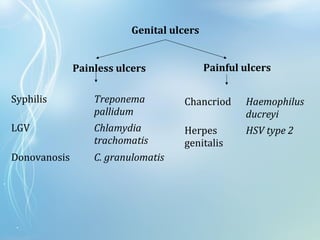


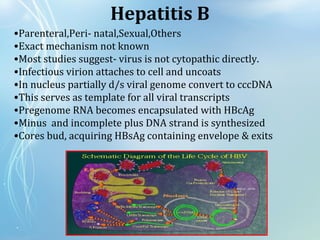
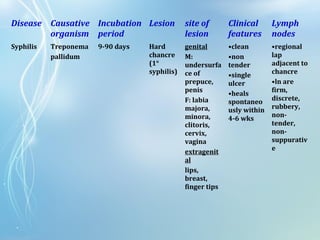
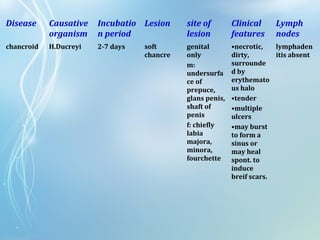

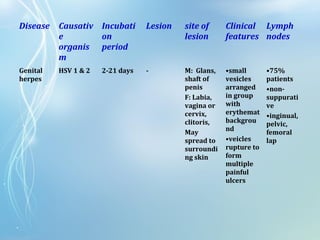

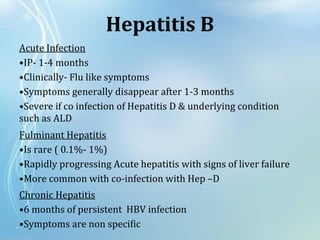
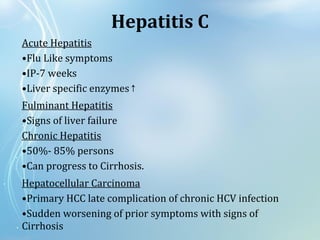






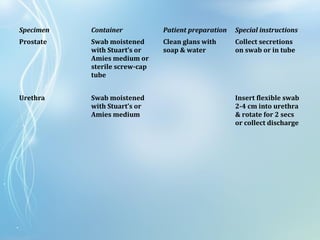


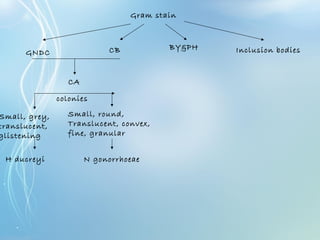
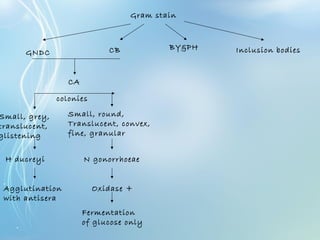
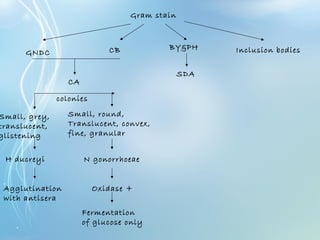
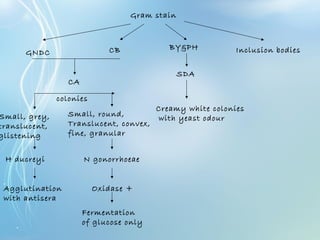
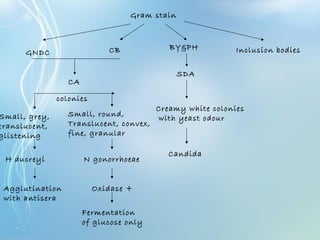
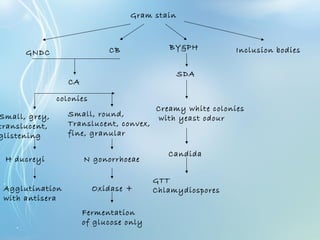
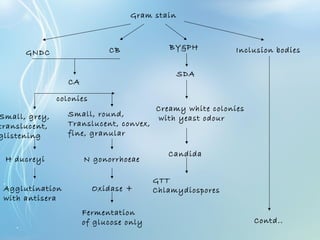
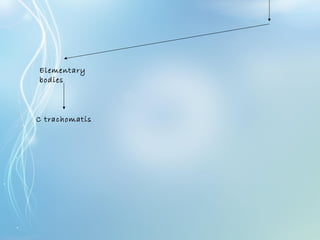

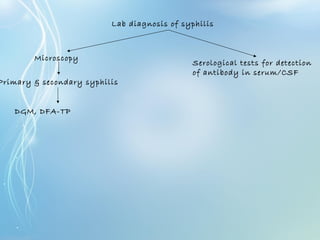
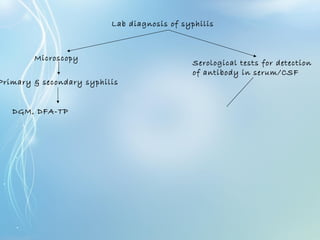
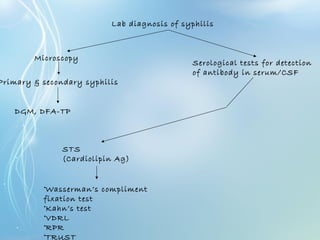
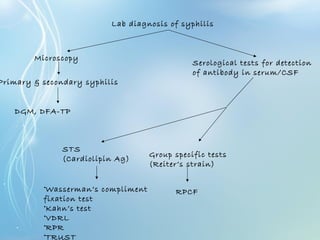
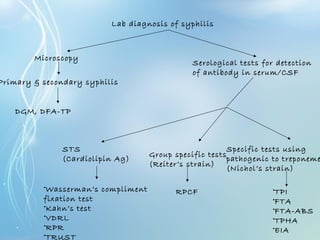
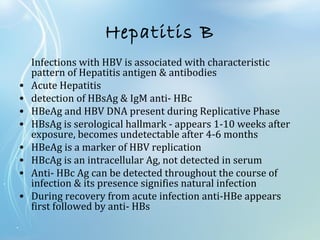
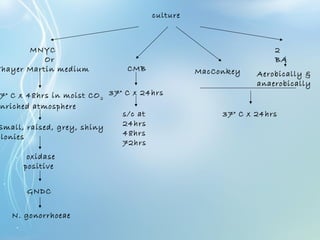
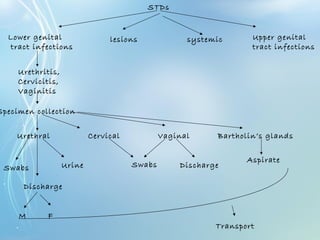
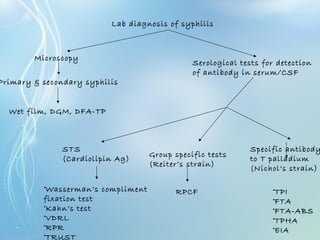

This document discusses sexually transmitted diseases (STDs). It defines STDs as communicable diseases predominantly transmitted through sexual contact and caused by bacteria, viruses, fungi or parasites. It then discusses factors influencing STDs, populations at risk, common clinical presentations including genital ulcers and discharge, and various STDs like syphilis, chlamydia, herpes, HIV and hepatitis B and C. It also covers the etiology, pathogenesis, signs and symptoms, complications and methods of laboratory diagnosis for major STDs.