Downloaded 427 times






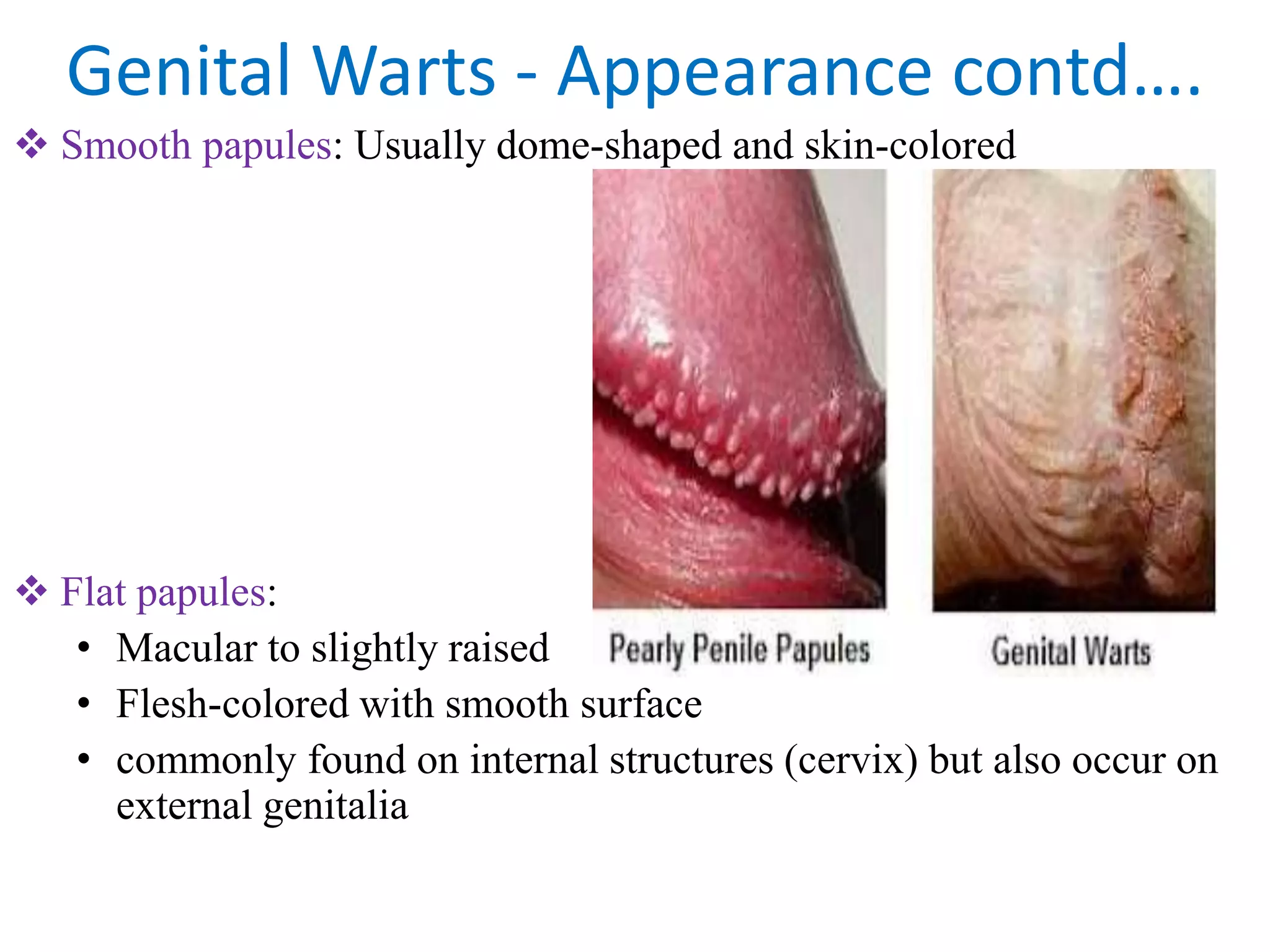














Genital warts are caused by certain types of human papillomavirus (HPV) that infect skin and mucous membranes of the genital area. There are over 100 types of HPV that can cause genital warts. The warts may appear as small bumps or groups of bumps in the genital region and can be itchy or painful. Diagnosis is usually made by visual examination with biopsy needed if uncertain. Treatment focuses on freezing, burning, or cutting off visible warts although they may recur. Prevention through HPV vaccination is recommended.