Learning Objectives: Atthe end of this unit, You
will be able to:
• List common STDs/STIs
• Elaborate ethological agents for STIs
• Identify epidemiology of STIs
• Identify clinical manifestation of STIs
• Identify general mode of transmission of STIs &
non-STIs
• Apply clinical & syndromic approach for managing
STIs
• State general preventive & control measures for
STIs
3.
Introduction
• The diseasesbelonging to this group are usually
transmitted during sexual intercourse so called
STDs/STIs
• At present there are more than 20 causes of STIs
• No single STIs can be regarded as an isolated
problem due to multiple infections are common
4.
Introduction …
• Multiplesexual partner (promiscuity) are a high–
risk group for STIs.
• They may be professional prostitutes, barmaids, or
persons who in other ways gain from casual sexual
relationships
• This group is called the promiscuous women pool
(PWP) most of them are unmarried, divorced or
widowed
• They are the reservoir of STIs
5.
Epidemiology of STIs:
•STIs are major public health problems in all
countries but more in developing countries where
inadequate diagnostic & treatment are available or
non-exit
• In Ethiopia there is limited information on
incidence & prevalence of STIs
• Most STI patients are symptomatic and seek
treatment from traditional healers, pharmacists,
drug vendor shops & marketplaces
6.
Approaches to manageSTIs: Two approaches
1. Ethological approaches:
Advantage:
• Accurate diagnosis & treatment
• Proper use of antibiotics ( decrease over treatment
& antibiotic resistant)
• Better way to diagnose & treat asymptomatic
infections
Disadvantage:
• Need laboratory support & experts
• Expensive ( patients may not cure due to lab test
cost)
• Time consuming
7.
Approaches …
2. Syndromicapproaches:
Advantage:
• Treatment given immediately
• Mixed infections may exist & may addressed
• No need of laboratory diagnosis
• Treated by mid-level health professionals
• Good approach for resource limited settings
Disadvantage:
• Over treatment with antibiotics leads to drug
resistance & decreased compliance
• Increase cost of drugs
• Asymptomatic infection is missed
8.
Risk factors are:
1.Age: 15 years & older
2. Marital status: unmarried people who often change
their sexual partners are more frequently exposed
3. Occupation: Soldiers, Drivers, Policemen,
students, seasonal laborers & other people who are
temporarily away from home tend to expose
themselves more easily
4. Residence: Due to industrialization & urbanization
there is usually a large group of single young men
& women in towns
5. Promiscuity
9.
Risk assessment ofSTIs:
• Sexual orientation & practice
• Number of recent & current sexual partners
• History of STIs in the patient
• Recent history of the partner
• Sociodemographic & other markers of high risk
(Occupation)
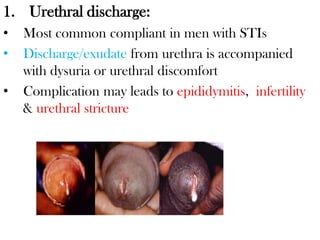
1. Urethral discharge:
•Most common compliant in men with STIs
• Discharge/exudate from urethra is accompanied
with dysuria or urethral discomfort
• Complication may leads to epididymitis, infertility
& urethral stricture
12.
Ethicology of urethraldischarge/ Urethritis:
A. Gonococcal urethritis cased by Neisseria gonorrhea
• Has short incubation period of 2-3 days
• Most have abundant & purulent discharge
• Have sever STI symptoms like dysuria, urgency &
frequency
B. Non gonococcal Urethritis/NGU:
• Usually caused by chlamydia trachomatis
• Has scanty to moderate, white, mucoid or serous
discharge
• Mild UTI symptoms
• Has long incubation period (1-3 weeks)
13.
Ethiology of urethraldischarge/ Urethritis…
• Quantity & appearance of discharge used to
distinguish accurately gonococcal & non gonococcal
urethritis in about 75-80% who are not urinated
recently but not show dual infection
• So that milking of urethra may be necessary to get a
more amount of discharge sample
Laboratory:
• Microscopy of urethral discharge stained with
methylene blue or safranin or Grams stain shows
pus cells with intracellular coffee bean shaped
diplococci >> N. Gonorrhea
• Pus cells without intracellular diplococci >> NGU
14.
Recommended treatment forurethral discharge
Ciprofloxacin 500 mg po stat
Or
Spectinomycin 2 grams IM stat
PLUS
Doxycycline 100 mg po bid for 7 days
Or
Tetracycline 500 mg qid for 7 days
Or
Erythromycin 500mg qid for 7 days if the patient
has contraindications for tetracycline (children,
pregnancy)
14
3/28/2024 STI
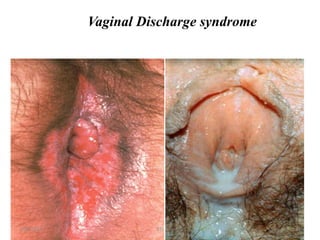
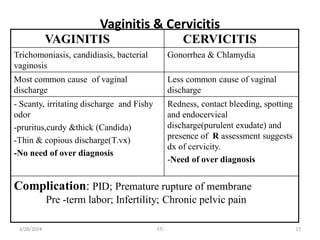
Vaginitis & Cervicitis
VAGINITISCERVICITIS
Trichomoniasis, candidiasis, bacterial
vaginosis
Gonorrhea & Chlamydia
Most common cause of vaginal
discharge
Less common cause of vaginal
discharge
- Scanty, irritating discharge and Fishy
odor
-pruritus,curdy &thick (Candida)
-Thin & copious discharge(T.vx)
-No need of over diagnosis
Redness, contact bleeding, spotting
and endocervical
discharge(purulent exudate) and
presence of R assessment suggests
dx of cervicity.
-Need of over diagnosis
Complication: PID; Premature rupture of membrane
Pre -term labor; Infertility; Chronic pelvic pain
17
3/28/2024 STI
18.
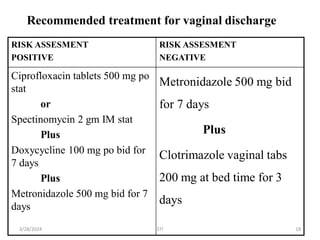
Recommended treatment forvaginal discharge
RISK ASSESMENT
POSITIVE
RISK ASSESMENT
NEGATIVE
Ciprofloxacin tablets 500 mg po
stat
or
Spectinomycin 2 gm IM stat
Plus
Doxycycline 100 mg po bid for
7 days
Plus
Metronidazole 500 mg bid for 7
days
Metronidazole 500 mg bid
for 7 days
Plus
Clotrimazole vaginal tabs
200 mg at bed time for 3
days
18
3/28/2024 STI
Genital Ulcer:
• Itis a loss of continuity of the skin of the genitalia
• May be painful or painless
• Frequently accompanied by inguinal
lymphadenopathy
Etiological agents of genital ulcers:
A. Treponema pallidum ( Syphilis)
B. Haemophilus ducreyi ( Chancroid)
C. C. trachomatis L1-L3 (Lymphogranuloma venerum or LGV)
D. Clamato bacterium granulomatous ( Granuloma Inguinale)
C &D are not common
A. Herpes simplex virus 1 or 2 /HSV( Genital herpes)
21.
A. Syphilis:
• Itis hard chancre which is painless
• A small popular lesion that rapidly ulcerates to
produce a non-tender indurated lesion with a clean
base & raised margins called Chancre
• Chancre may occur at any point of contact (
genitalia, anus, mouth, lips)
• Heal without treatment with in 1-6 weeks
• Swollen lymph nodes may appear
22.
Clinical Manifestation: Threestages of syphilis:
A. Primary syphilis:
• Consists of hard chancre, the primary lesion
of syphilis, together with regional
lymphadenitis
• The hard chancre is a single, painless ulcer on
the genitalia or elsewhere (lips, tongue,
breasts) & heals spontaneously in a few weeks
without treatment
• The lymph glands are bilaterally enlarged
and not painful
• There will not be suppuration
23.
B. Secondary syphilis:
•After 4 – 6 weeks of the primary infection, a
generalized secondary eruption appears, often
accompanied by mild constitutional
symptoms
• These early rashes tend to be symmetrical,
quickly passing, and do not itch
• These early skin lesions are highly infective
and many spirochetes are demonstrated in
them
24.
C. Tertiary syphilis:
•This stage is characterized by destructive,
non-infectious lesions of the skin, bones, viscera,
and mucosal surfaces.
• Other disabling manifestations occur in the
cardiovascular system (aortic incompetence,
aneurysms) or central nervous system (dementia
paralytica, tabes dorsalis).
NB:-
Syphilis in pregnancy- According to the severity,
congenital syphilis can result in congenital
abnormalities, still birth, or repeated spontaneous
abortions.
25.
Diagnosis
• Serologicaltest – will be positive 6 to 8 weeks
after infection
• Dark field microscopy of smears from primary
lesion (hard chancre) or from skin lesions in the
early secondary stage will show the spirochaetes
Complications of syphilis:
• Secondary syphilis
• Aortitis with valvulitis
• Neuro syphilis
26.
B. Chancroid
• Causedby Hemophilus ducreyi
• Incubation period 3-15 days
• Ulcer on penile shaft or prepuce
• It is Soft chancre which is painful
• The painful progressive from small papule to pustule
and then ulcer with soft margins described as soft
chancre, yellow gray discharge covering & erythema
• Inguinal adenopathy becomes necrotic & fluctuant
(bubo) follows the ulcer with in 1-2 weeks
Complication:
• Penile autoamputation
27.
E. Genital Herpes:
•HSV virus has two types
1. HSV-1 causes dominantly oral disease
2. HSV-2 causes dominantly genital disease
• Worldwide the most common cause of genital ulcer
• Latency & frequent recurrence characterizes genital
herpes , producing a lifelong infection /persistent
28.
Herpetic ulcers:
• Areusually painful and multiple
• Starts as clear vesicle and becomes pustule, which later
erodes to an ulcer and then crusts
• Heals spontaneously after 2-3 weeks
• Recurrence possible but milder
• It tends to be aggressive in HIV patients with extensive
tissue involvement and chronic ulceration.
• It may also be dissemination to CNS, skin etc
Complications:
• Recurrence
• Aseptic meningitis and encephalitis
29.
Management of GenitalUlcer
1. When specific Etiologic diagnosis is made
Syphilis:
A. Primary & secondary syphilis
• Benzathin penicillin 2.4 M IU Im stat or
• Tetracycline or Erythromycin 500mg PO Qid for 2
weeks for penicillin sensitive people
B. Tertiary syphilis
• Benzathin penicillin 2.4 M IU Im single dose every week for
3 consecutive weeks or
• Tetracycline or Erythromycin for one month for
penicillin sensitive individuals
C. Early congenital syphilis
• Crystalline penicillin 50,000 IU/ Kg per dose IV or Im bid in
the first 7 days of life and Tid then after for 10- 14 days
30.
Management of GenitalUlcer
1. When specific Etiologic diagnosis is made
Genital Herpes:
• Acyclovir 200 mg 5X per day for 10 days or
• Acyclovir 400 mg Po TID for 10 days
31.
Management of GenitalUlcer
1. When specific Etiologic diagnosis is made
Chancroid:
• Ceftriaxone 250mg 1M stat or
• Erythromycin 500mg PO TID for 7 days
LGV:
• Doxycycline 100mg PO BID for 14 days or
• Tetracycline 500mg PO QID for 14 days
Granuloma Inguinale:
• Cotrimoxazole 02 tab PO BID for 14 days
N.B: Tetracycline is contraindicated during
pregnancy
32.
2. When specificEtiologic diagnosis is not made –
Syndromic approach
A. For non-vesicular genital ulcer:
• Benzathine penicillin 2.4million IU IM stat Or
• (if penicillin allergy) Doxycycline 100mg PO BID
for 14 days Plus
• Ciprofloxacin 500 mg PO for 3 days or
• Erythromycin 500mg PO QID for 7 days
33.
2. When specificEtiologic diagnosis is not made –
Syndromic approach …
B. For Vesicular, multiple or recurrent genital ulcer:
• Acyclovir 200 mg 5X per day for 10 days or
• Acyclovir 400 mg Po TID for 10 days
Recommended treatment for:
I. Recurrent Infection: Acyclovir 400 mg Po TID for
5 days
II. Suppressive therapy: Acyclovir 400 mg PO BID
continuously
34.
4. Lower abdominalpain:
• In women is associated with pelvic inflammatory
disease (PID).
• PID caused by microorganisms ascending from
lower genital tract in women which includes:
o Salpingitis ( inflammation of fallopian tubes)
o Endometritis(inflammation of endometrium)
o Parametritis( inflammation of parametrium)
o Oophoritis ( Inflammation of ovaries)
35.
Etiology of PID:
•CommonlyN. gonorrhea & C. trachomatis (STIs)
•PID may due to Mycoplasma, Bacteroides,
Streptococcus, E. Coli, H. Influenza (Non STIs)
Risk factors of PID:
•STD
• Postpartum & post abortal ascending infections
• Intra uterine device ( IUD)
36.
Clinical feature:
• Mildto severe bilateral lower abdominal pain is the
most common complaint,
• May first be noticed during or shortly after the
menses & which is sometimes associated with fever
• The presence of vaginal discharge supports the
diagnosis of PID &
• Pain during intercourse or urination may also be
present
37.
Physical examination
• Lowerabdominal & adnexal tenderness together
with cervical excitation tenderness may be indicative
of PID
• A tender pelvic mass together with fever, nausea or
vomiting can also be detected
• Vaginal discharge, genital ulcer, presence of IUD,
open cervix (abortion tissue seen or felt) support the
diagnosis of PID
38.
Diagnosis:
• It isoften difficult.
• Over diagnosis & treatment may be justified in order
to prevent complications
• Rule out other cause of lower abdominal pain in
women such as appendicitis , ectopic pregnancy &
Cholecystitis
Laboratory:
• Direct wet mount microscopy of a vaginal specimen
is necessary
• The presence of pus cells in numbers exceeding
those of epithelial cells suggests infection of the
lower genital tract
39.
Complications:
• Peritonitis andintra-abdominal abscess
• Adhesion and Intestinal obstruction
• Ectopic Pregnancy
• Infertility
Treatment:
• Most patients with mild to moderate PID can be
treated as an out patient
• Some patients need hospital admission
Recommended treatment forPID at outpatient:
• Ciprofloxacin 500 mg PO stat OR
• Spectinomycin 2gm IM stat Plus
• Doxycycline 100 mg PO BID for 14 days Plus
• Metronidazole 500mg Po ID for 14 days
Admit the patient if there is no improvement within
72 hours
42.
Recommended treatment forPID at in patient:
• Metronidazole 500mg Po ID for 7 days Plus
• Clotrimazole vaginal tabs 200mg at bed time for 3
days
Non Specific: Adequate bed rest, analgesic,
If there are any obstetric or surgical complications,
refer the patient as early as possible
43.
5. Inguinal bubo:
•Inguinal bubo is an enlargement of the lymph glands
in the groin area.
• Etiology:
o C.trachomatis serovar L1-L3 (Lymphogranuloma
venereum or LGV)
o Haemophilus ducreyi (chancroid)
o Calymmato bacterium granulomatis (granuloma
inguinale)
o Treponema pallidum (syphilis) may sometimes
cause inguinal bubo
44.
• Except incase of LGV, a bubo is rarely a sole
manifestation of STD and is usually found together
with the etiologically related genital ulcer.
• Non-sexually transmitted local or systemic infections
can also cause inguinal lymphadenopathy.
Clinical feature:
• Usually patients complain of unilateral or bilateral
painful swelling in the groin, but buboes can be
painless.
• It is important to ask for any history of associated
genital ulcer.
45.
Treatment:
Recommended treatment forInguinal Bubo:
• Ciprofloxacin 500 mg PO BID for 3 days PLUS
• Doxycycline 100 mg PO BID for 14 days OR
• Erythromycin 500 mg PO BQID for 14 days
• Fluctuant buboes require aspiration through
adjacent healthy skin (don’t incise for drainage).
• If genital ulcers are present, treat with the
etiologically related cause of the ulcer.
46.
6. Scrotal SwellingSyndrome
• Cause of scrotal swelling depend on age of patient
A. For those younger than 35 years
• N. gonorrhoeae
• C. trachomatous
B. For those older than 35 years
• Gram negative organisms
• Tuberculosis
• Other cause include: Brucellosis, Mumps,
Onchocerciasis, Wuchereria buncrofti
47.
6. Scrotal SwellingSyndrome …
• Exclude other causes of scrotal swelling which may
require urgent surgical evaluation & management
o Testicular Torsion
o Trauma
o Incarcerated inguinal hernia
Complications of Scrotal Swelling: caused by STI:
• Epididymitis
• Infertility
• Impotence
• Prostatitis
48.
Recommended treatment forScrotal swelling
Treatment of Scrotal swelling suspected of STI
origin is similar to Urethral discharge
• Ciprofloxacin 500 mg PO stat OR
• Spectinomycin 2gm IM stat PLUS
• Doxycycline 100 mg PO BID for 7 days OR
• Tetracycline 500 mg PO QID for 7 days
• Supportive Treatment: Analgesia & scrotal support
may be indicated if the patient has severe pain
49.
General mode oftransmission of STIs:-
• Mainly sexual /Genital, Anal, oral (Almost all STIs)
• Accidentally by touching infective tissues(Genital herpes,
Candidiasis, Trichomoniasis & Syphilis)
• Blood transfusion
• Congenitally before birth (Genital herpes, Candidiasis,
Trichomoniasis & Syphilis)
• Transmission to the neonate usually occurs via the infected
birth canal ( Genital herpes, Candidiasis, Trichomoniasis &
syphilis)
• Indirectly through contact with contaminated articles clothes
(Genital herpes, Candidiasis, Trichomoniasis & Syphilis)
50.
General prevention &control methods of STIs:
1. Partner notification & management
2. Case detection & treatment with sexual partner
3. Counselling on Condom utilization & supply
4. Educate public to seek medical help whenever there is any
complain related to STIs
5. Abstain from sexual intercourse until investigation &
treatment of self & partners are completed
6. Health education & risk reduction counselling ( ABC rules)
7. Linkage with HIV counselling & testing
8. Follow up visits for patients with STIs