Downloaded 48 times

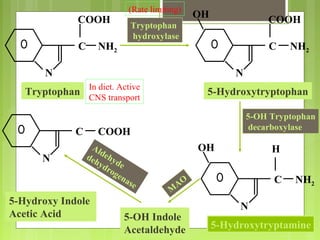
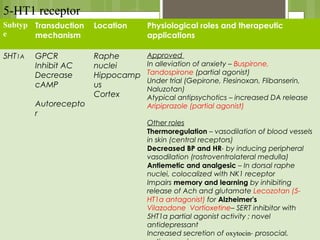
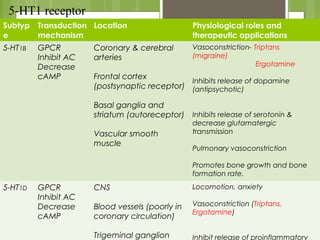
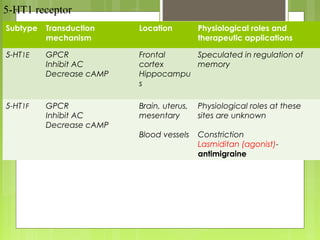
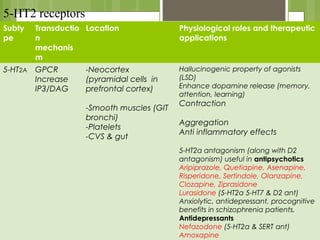
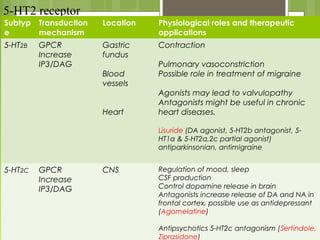
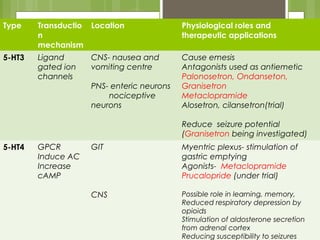
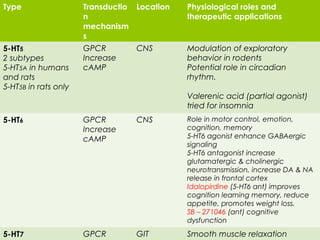
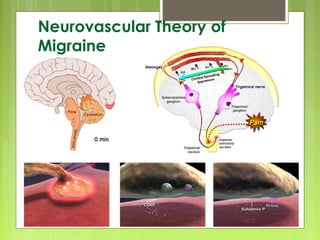


The document discusses serotonin, its biochemical properties, synthesis, metabolism, and its roles in various physiological processes and diseases. It outlines the history of serotonin research, details several receptor subtypes and their therapeutic applications, and explores connections between serotonin and conditions like migraines and depression. Additionally, it highlights the mechanisms of action for different drugs affecting serotonin levels and describes serotonin syndrome as a potentially dangerous condition resulting from drug interactions.





































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















