Downloaded 37 times

![Synthesis
[Rate limiting step]](https://image.slidesharecdn.com/serotonin-200807081835/85/Serotonin-3-320.jpg)
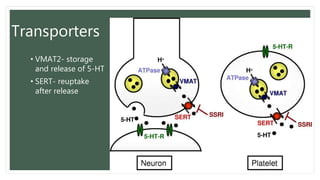
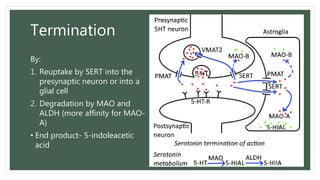
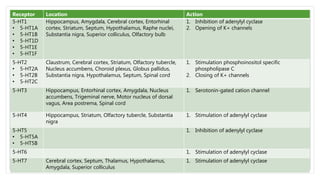
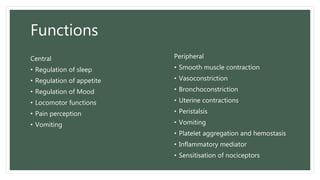
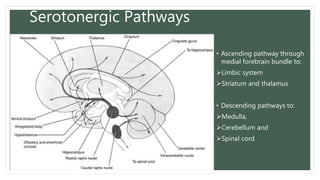
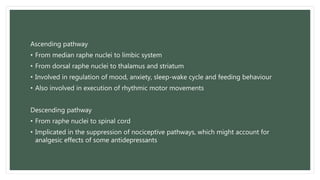
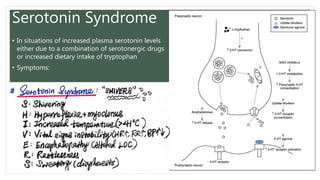
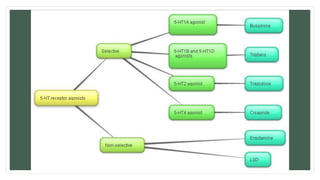
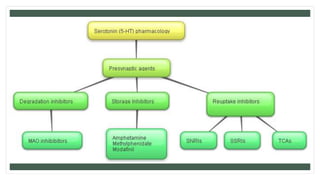
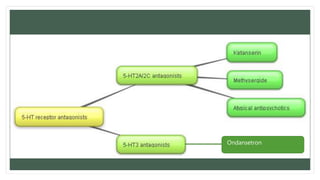
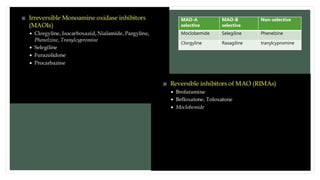
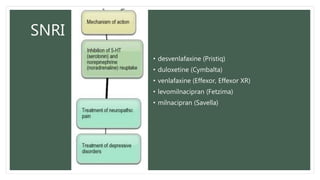
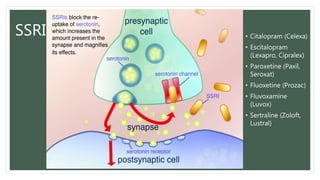
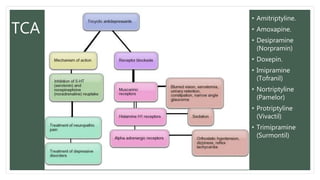

Serotonin is a neurotransmitter that plays an important role in many physiological and psychological functions. It is synthesized from tryptophan and transported into presynaptic neurons by VMAT2. After release, it is terminated by reuptake via SERT or degradation by MAO and ALDH. Serotonin receptors are located throughout the brain and body. Serotonin is implicated in various psychiatric conditions like depression, anxiety, OCD, schizophrenia, and personality disorders. Drugs that affect serotonin levels, like SSRIs, SNRIs, TCAs, and MAOIs, are used to treat many of these disorders.





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












