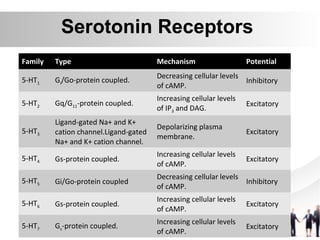
Serotonin is a neurotransmitter synthesized from tryptophan. It activates G protein-coupled serotonin receptors and ligand-gated ion channels. Serotonin is involved in various physiological processes like respiration, gastrointestinal motility, cardiovascular function, and central nervous system functions such as mood, sleep, and pain perception. Migraine is a neurological disease characterized by recurrent moderate to severe headaches. Treatment involves acute medications for mild attacks and prophylactic drugs like beta-blockers for more frequent attacks.


























![Serotonin Pharmacology (5-HT) [Neurotransmitter]](https://cdn.slidesharecdn.com/ss_thumbnails/07-210419085115-thumbnail.jpg?width=640&height=640&fit=bounds)

























































![5 HT [seratonin]](https://cdn.slidesharecdn.com/ss_thumbnails/5-htseratonin-210709174110-thumbnail.jpg?width=640&height=640&fit=bounds)




















