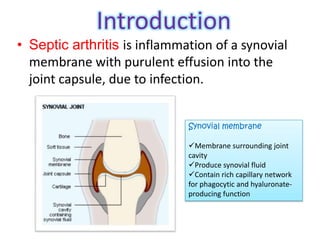
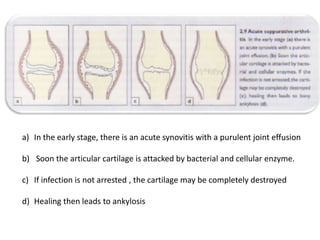
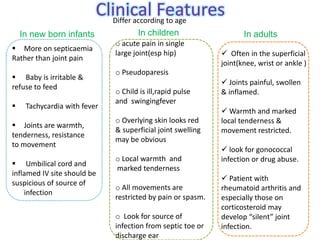
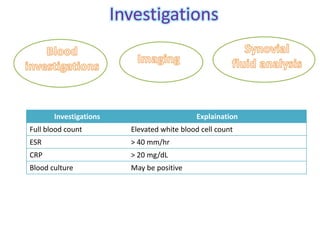
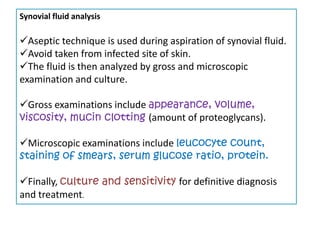
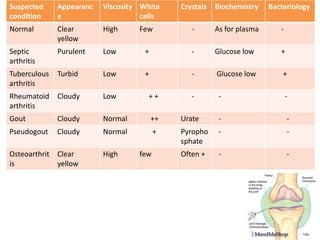
Septic arthritis is a joint infection caused by bacteria or other microbes entering the joint space. It leads to inflammation of the synovial membrane and purulent effusion. Common symptoms include pain, swelling, warmth and limited movement of the infected joint. Diagnosis involves synovial fluid analysis showing purulence and leukocytosis, along with supportive blood tests. Treatment is with antibiotics and surgical drainage may be needed. Complications can include bone and cartilage destruction, joint deformity, and secondary osteoarthritis.