This document discusses septic arthritis, including its definition, risk factors, common causative organisms, modes of infection, pathogenesis, clinical features, investigations, treatment, and approaches to joint aspiration and drainage. The key points are:
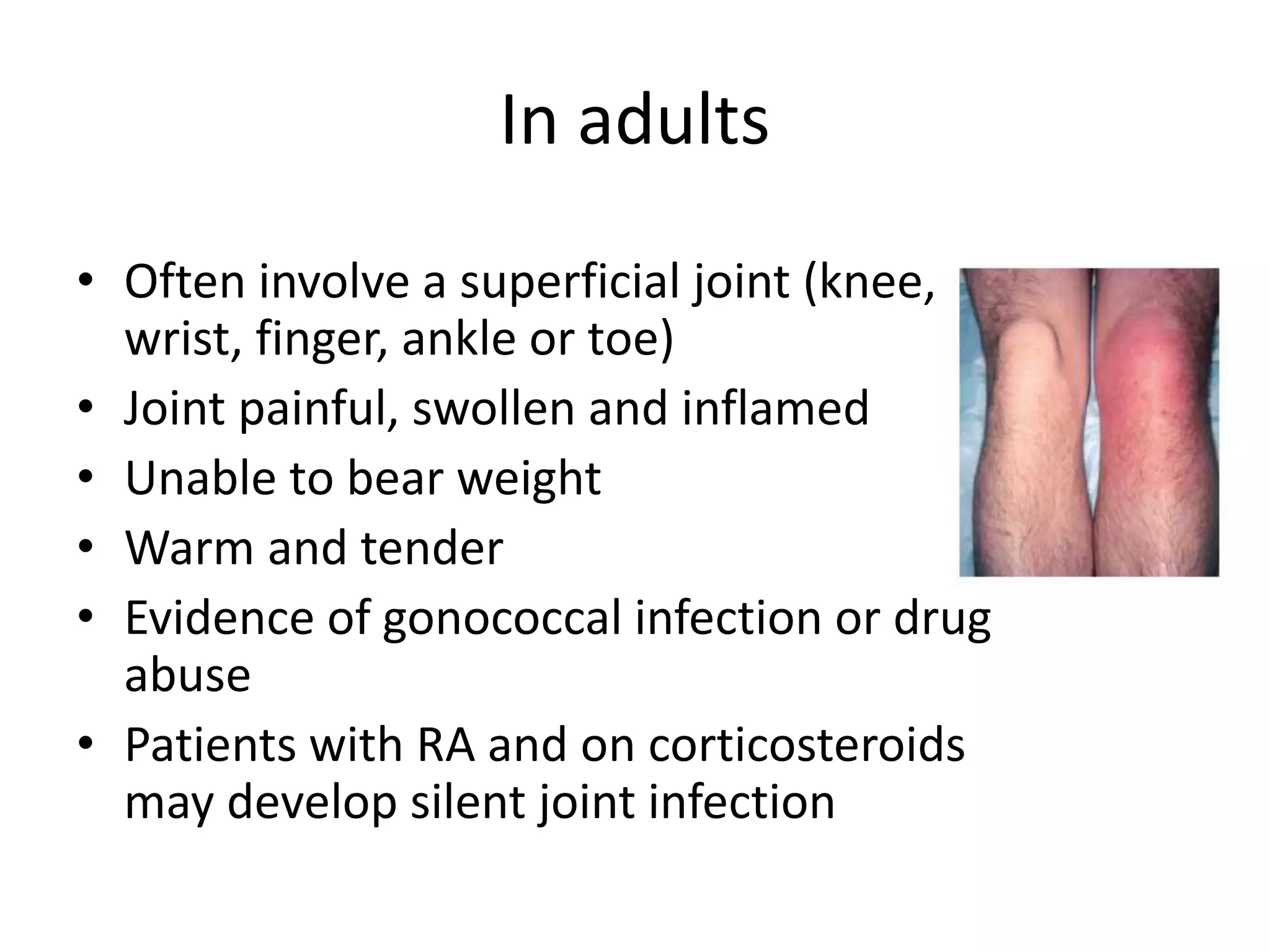
- Septic arthritis is a joint infection caused by bacterial invasion of the synovial membrane. It commonly affects the knee, hip, shoulder and ankle.
- Risk factors include rheumatoid arthritis, prosthetic joints, IV drug use, and diabetes. Common organisms include Staphylococcus aureus and gram-negative bacilli.
- Treatment involves joint drainage, IV antibiotics based on culture and sensitivity results, and splinting the joint. Surgical drainage is often needed if