Downloaded 575 times
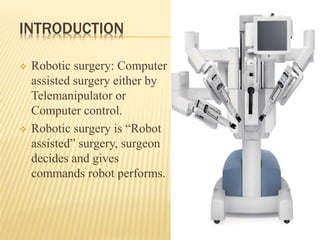

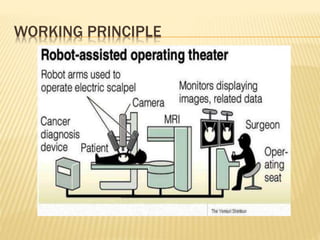
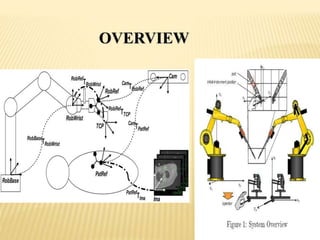

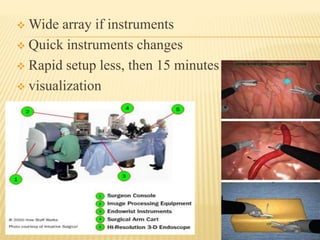


The document discusses robotic surgery, detailing its history, working principles, advantages, and disadvantages. It emphasizes the evolution of robotic systems from the late 1980s to recent technologies, outlining the various types of surgical systems and their functionalities. A case study highlights a minimally invasive liver resection as an example of successful robotic surgery while also addressing safety concerns and the need for further evaluation of cost-effectiveness.






















































































