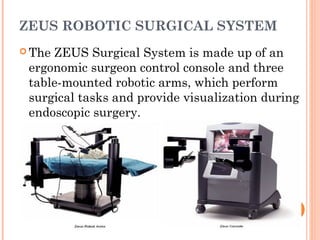
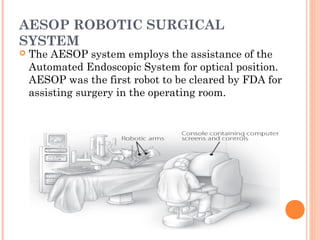
This document discusses robotic surgery, providing details on its history, current systems, and advantages. Robotic surgery uses robots to assist surgeons by allowing them to view organs being operated on through cameras inserted into the body and manipulate surgical instruments remotely via a control panel. Three major robotic surgery systems are discussed - the da Vinci Surgical System, ZEUS Robotic Surgical System, and AESOP Robotic Surgical System. Robotic surgery provides benefits like enhanced views, smaller incisions, less scarring and blood loss, and faster recovery times for patients compared to open surgery. However, robotic surgery systems are still relatively expensive to purchase and implement.