Robotic surgery uses robotic systems to assist surgeons with complex procedures. Some key points:
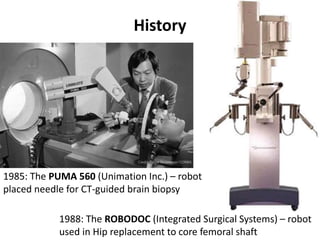
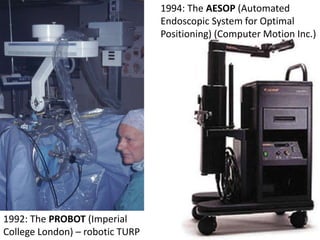
- Early systems included ROBODOC in 1985 for hip replacements and AESOP in 1994 for positioning the endoscope. The Da Vinci system, introduced in 2000, is now the most widely used system.
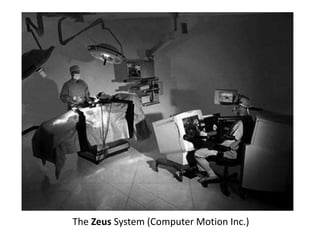
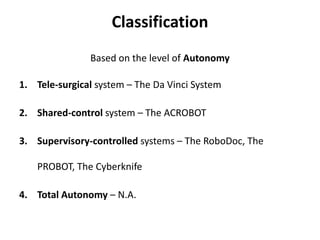
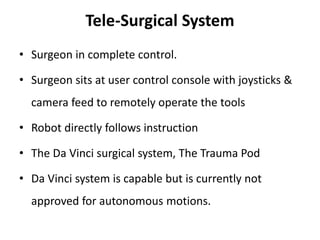
- Systems can be tele-surgical like Da Vinci where the surgeon controls the robot remotely, shared-control where the robot provides feedback, or supervisory where the robot executes pre-planned motions autonomously under surgeon oversight.
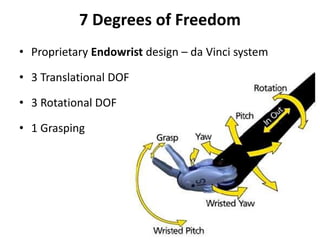
- The Da Vinci system allows the surgeon to sit at a console several feet from the patient with magnified 3D HD vision and wristed instruments that mimic hand movements with