Downloaded 36 times
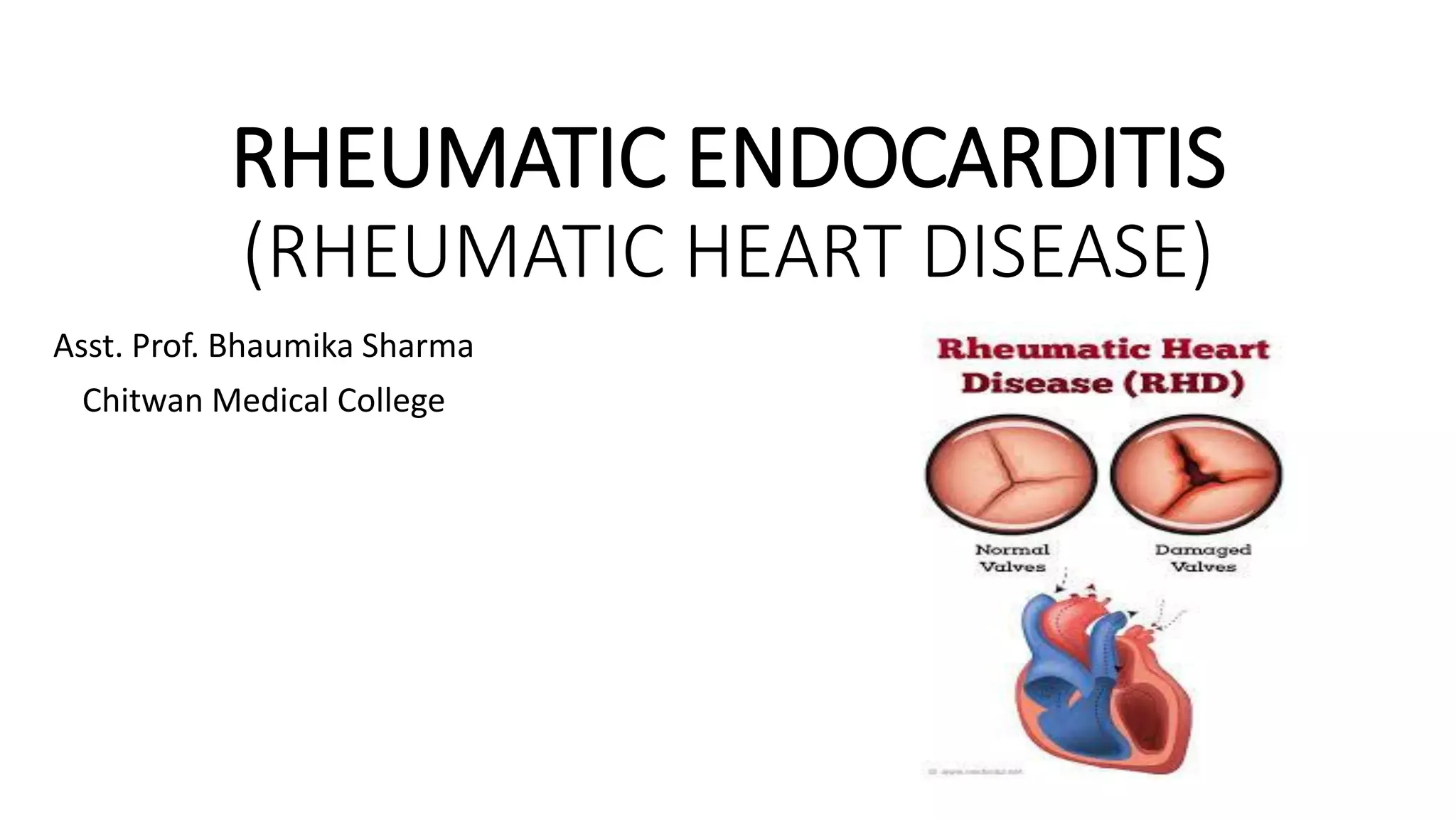















































Rheumatic heart disease is caused by an autoimmune reaction to strep throat infection. It involves inflammation of the heart valves and can lead to valve damage over time. The mitral and aortic valves are most commonly affected, resulting in stenosis or insufficiency. Symptoms may include fever, joint pain, or heart murmurs. Treatment involves antibiotics to prevent recurrence, along with medications, activity restriction, and possibly valve surgery for severe cases. Nursing care focuses on reducing fever, monitoring the heart for changes, limiting activity, and educating patients and their families.