Download to read offline
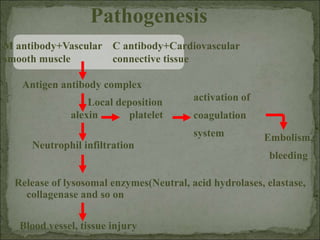
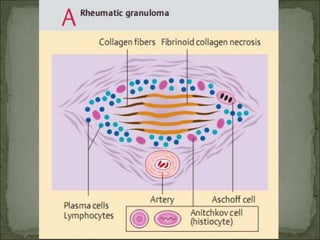
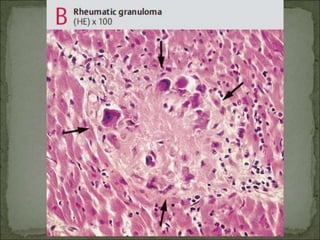
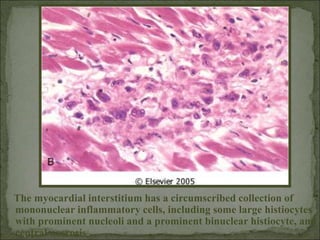
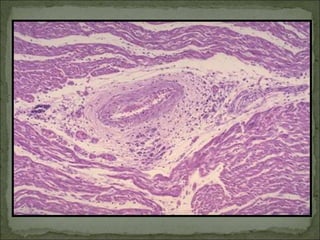
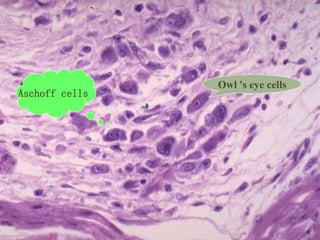
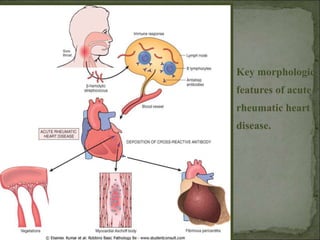

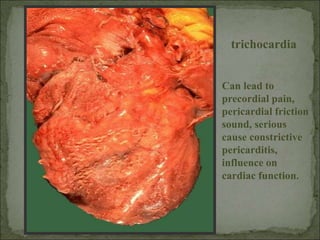



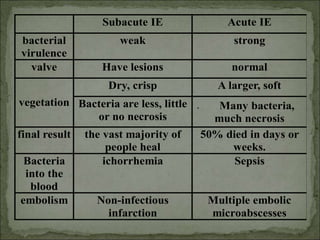
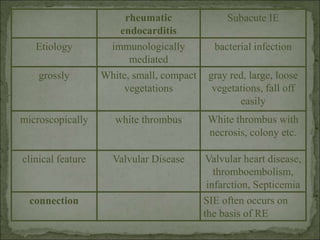

Rheumatic fever and rheumatic heart disease are conditions that can occur after a streptococcal throat infection. Rheumatic fever is an inflammatory disease that affects the heart, joints, skin, and blood vessels. It is characterized by lesions called Aschoff bodies and rheumatic granulomas. Long term, it can lead to rheumatic heart disease where the heart valves are damaged. The disease process involves an immune response to streptococcal antigens that causes inflammation and tissue damage. Symptoms vary by the organs involved but can include fever, arthritis, heart valve abnormalities, and skin rashes.























































































