Downloaded 256 times
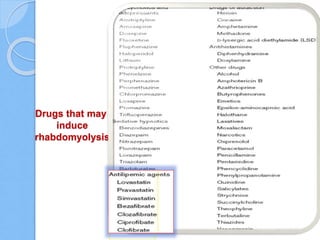

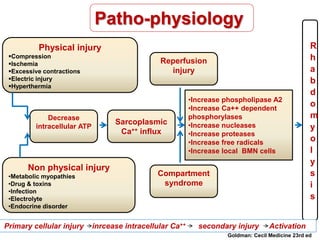
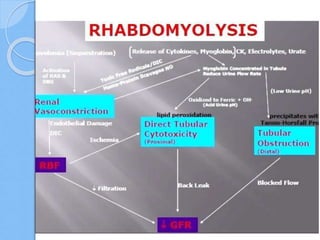
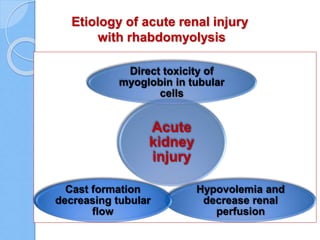
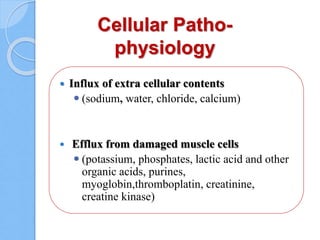
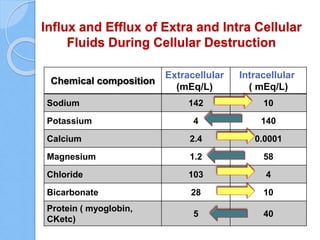
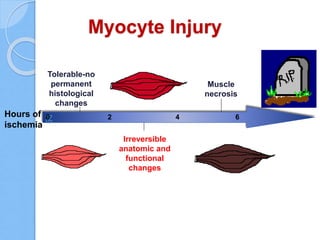
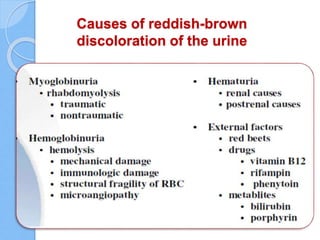
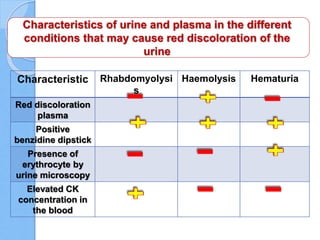
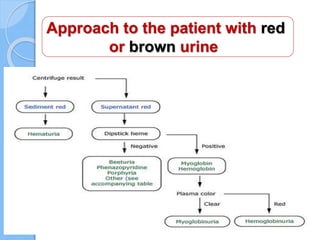
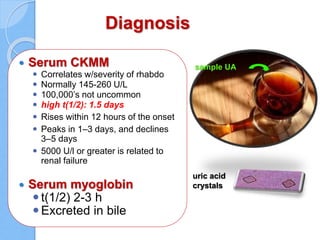





Rhabdomyolysis is the destruction or breakdown of skeletal muscle fibers that results in the release of intracellular contents into the bloodstream. The document discusses various causes of rhabdomyolysis including physical trauma, excessive exertion, infections, drugs, toxins, and metabolic disorders. It also describes the pathophysiology involving decreased ATP production and increased intracellular calcium levels leading to muscle cell damage. Diagnosis involves elevated creatine kinase and presence of myoglobin in urine or blood. Treatment focuses on aggressive fluid resuscitation to prevent acute kidney injury from myoglobin toxicity, along with urine alkalinization and potentially mannitol diuresis.























































































