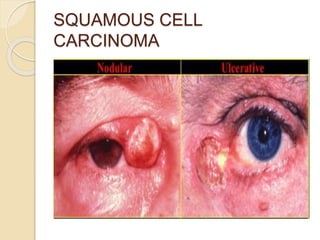
This document discusses different types of eyelid tumors. It first separates tumors into benign and malignant categories. Common benign tumors include papillomas, xanthelasma, hemangioma, and neurofibroma. The most frequent malignant tumors are basal cell carcinoma, squamous cell carcinoma, sebaceous gland carcinoma, and malignant melanoma. For each tumor type, the document describes characteristics such as appearance, patient demographic, treatment options, and clinical features.