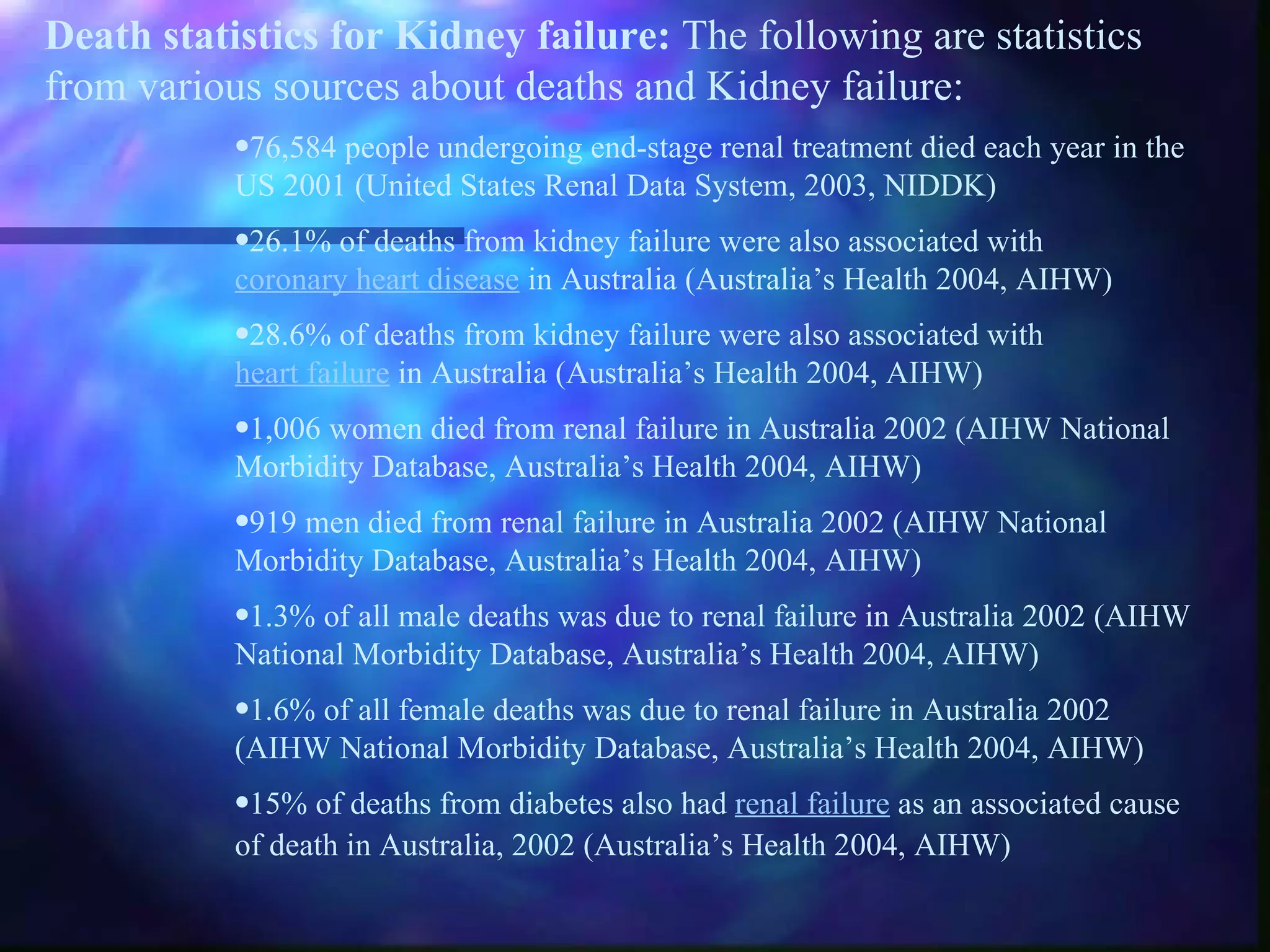
The document discusses renal failure and its relationship to cardiovascular disease. It provides statistics on the prevalence, incidence, and mortality rates of renal failure in the US and Australia. It then covers topics such as the structure and function of the kidneys, classification of renal failure, its effects on the cardiovascular system, and approaches to treatment including dialysis, transplantation, and their risks.