Downloaded 69 times

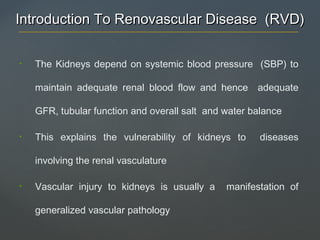
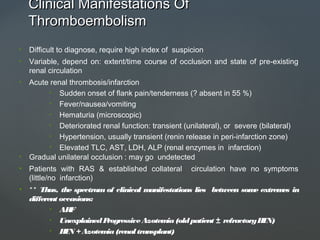


![a. Gross appearance of benign nephrosclerosis - Fine, leathery granularity
b. Hyaline arteriolosclerosis. [arterioles with hyaline deposition, marked thickening of
walls and narrowed lumen] & interlobular and arcuate arteries show medial
hypertrophy, replication of internal elastic lamina and increased myofibroblastic
tissue in intima [Fibroelastic hyperplasia]](https://image.slidesharecdn.com/renovasculardisease-180710155200/85/Renovascular-disease-16-320.jpg)

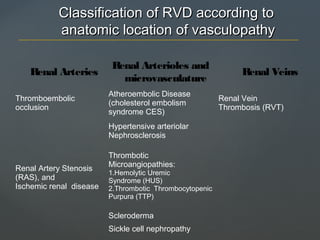
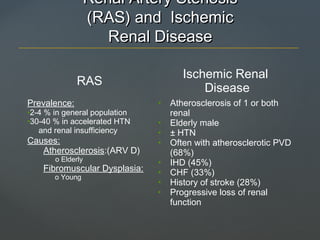
![a. Fibrinoid necrosis of afferent arteriole [PAS stain] – Cytologic detail lost,
Smudgy eosinophilic appearance of vessel wall.
b. Hyperplastic arteriolitis (onion-skin lesion) [intimal thickening by proliferation of
elongated, concentrically arranged smooth muscle cells, together with fine
concentric layering of collagen and accumulation of pale-staining material that
represents deposition of proteoglycan and plasma protein ]](https://image.slidesharecdn.com/renovasculardisease-180710155200/85/Renovascular-disease-18-320.jpg)
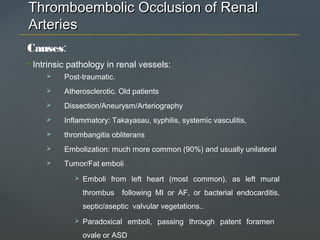
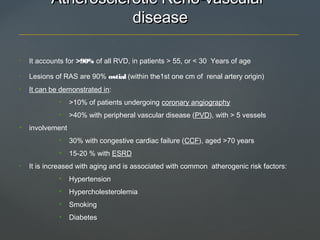
![Fibrin stain showing platelet-fibrin thrombi in the glomerular capillaries [Characteristic
feature]](https://image.slidesharecdn.com/renovasculardisease-180710155200/85/Renovascular-disease-20-320.jpg)





Renovascular diseases (RVD) involve pathology affecting the renal vasculature, leading to impaired renal function, hypertension, and related conditions. Key types include renal artery stenosis, fibromuscular dysplasia, atheroembolic disease, and thrombotic microangiopathies, each with distinct causes, clinical manifestations, and prognoses. Diagnosis and management require careful consideration of underlying conditions and may involve interventions to restore renal blood flow.


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
