ข้อแนะนาจาก Health EducationAuthority 1)
ควรออกกาลังกายด้วยความหนักปานกลาง เช่น การเดินเร็วๆ 30 นาที อย่างน้อย 5 ครั้ง
ต่อสัปดาห์ ซึ่งการเดินอาจเดินทีเดียว 30 นาที หรือเดิน ครั้งละ 15 นาที หลายๆ ครั้ง
ข้อแนะนาจาก US Center for Disease Control and Prevention 2)
ทุกคนควรออกกาลังกายด้วยความหนักปานกลาง เช่น การเดินเร็วๆ 30 นาทีเกือบทุกวัน
ข้อแนะนาจาก Quebec Consensus Conference3)
เพื่อสุขภาพทีดี การออกกาลังกายควรใช้กล้ามเนื้อกลุ่มใหญ่ออกกาลังกายด้วยความหนัก
่
มากกว่าปกติ ใช้พลังงานอย่างน้อย 700 กิโลแคลอรีต่อสัปดาห์ โดยทาบ่อยๆ เช่น เกือบทุก
วัน (ในทางปฏิบัติ การเดินเร็วๆ 20 - 30 นาทีก็พอแล้ว))
1) Killoran AJ, Fentem, P, Casperson C (eds), Moving on: International Perspectives on Promoting Physical Activity
(Health Education Authority: London, 1994).
2) Pate RR, Pratt M, Blair SN et al, Physical activity and public health: a recommendation from the Centers for Disease Control
and Prevention and the American College of Sports Medicine, JAMA (1995) 273:402-8.
3) Blair SN, Hardman A, Special issue: physical activity, health and well-being-an international consensus conference, Res Quart
Exerc Sport (1995) 66:4.
14.
ประโยชน์ของการออกกาลังกายเพื่อสุขภาพ (1)
การออกกาลังกายเพื่อสุขภาพมีประโยชน์หลายอย่าง* คือ
ลดความอ้วน (ไขมัน)
เพิ่มกล้ามเนื้อ (ทาให้น้าหนักอาจไม่ลด)
ลดไขมันในเลือด
เพิ่ม HDL ในเลือด HDL เป็นไขมันที่ดี จะช่วยปฺองกันโรคหลอดเลือดหัวใจตีบและ
อุดตัน HDL ยิ่งสูงมากจะยิ่งดี
สมรรถภาพการทางานของหัวใจจะดีขึ้นมากถ้าออกกาลังกายที่ถูกต้องอย่าง
สม่าเสมอ ชีพจรหรือหัวใจจะเต้นช้าลงซึ่งจะเป็นการประหยัดการทางานของหัวใจ
ปฺองกันและรักษาโรคเบาหวาน
W. Hollmann, et al 1988, p. 40 -48 . The Cardiovascular system in the Olympic Book of Sports Medicine, Volume I of
the Encylcopaedia of Sports Medicine. Ed. By A Dirix et al Blackwell Scientific Publications Oxford.
PRINCIPLE OF STROKEREHABILITATION
1. Holistic care
2. Interdisciplinary team care
: Patient, family
: Team conference
3. Goal- directed treatment
36.
Goal of Rehabilitation :
1. Minimize the impact of disability result
from the stroke
2. Optimize quality of life for both the
patient and the personal caregiver.
ควรมีผู้ป่วยหรือญาติ เข้าร่วมกาหนดเป้าหมาย
โดยอยู่บนพื้นฐานของความเป็นจริง
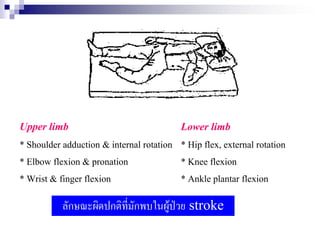
Motor recovery
- Sequenceof recovery can stop at Recovery of language and
any stage perceptual function
- Most : in the first 3 months * recovery usually occur
Minor : improve occur after 6 mons slower and over a more
post onset prolonged time course than
- Lower extremity function recover motor recovery
earliest and most completely * most aphasia recovery
followed by upper extremity and occur in the first 3 - 6 mons
hand function
- Proximal control precedes distal
control
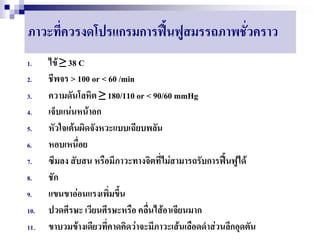
CANDIDATE FOR REHABILITATION
EVERYCASE WHEN :
• Medical stable 24-48 hrs : BP <180/110 mmHg
• No progressive stroke
Intensive program if
•follow 2 step command
•good cognitive
42.
“Rehabilitation in earlyphase”
Goals
Prevent complications from immobilization & deconditioning
Early activation/ remobilization
Patient and family education
Improve self care function
43.
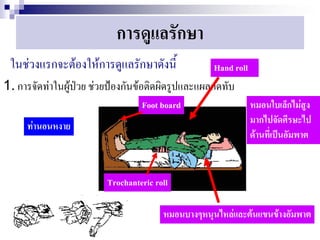
Rehabilitation program inearly phase
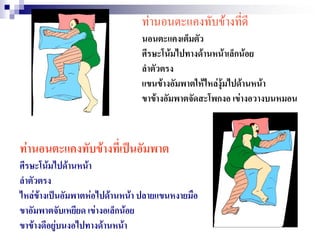
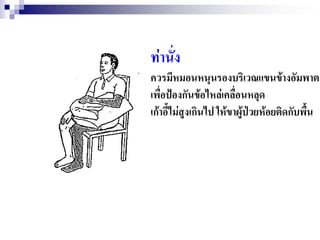
1. Proper bed and chair position
2. Frequent turn and position change
3. Deep breathing and cough exercise
4. Frequent skin inspection
5. Bed positioning and mobility
6. Bowel and Bladder care
เครื่องมือทางไฟฟ้าที่นามาใช้กับผู้ป่วย
ES (electrical stimulation) ใช้ติดในบริเวณที่กล้ามเนื้อ
อ่อนแรงเพื่อช่วยการคงพิสัยของข้อและช่วยป้องกันไม่ให้กล้ามเนื้อ
เหี่ยวลีบ
54.
ภาวะข้อไหล่เคลื่อน
พบได้ 50-80%
พบได้บ่อยในระยะแรกที่กล้ามเนื้ออ่อนแรงปวกเปียก
การแก้ไข
1. ใส่อุปกรณ์ช่วยพยุงหัวไหล่
2. ES (electrical stimulation)
3. การจัดวางแขนให้ถูกต้องเวลานั่ง หรือนอน
4. การออกกาลังกายเพื่อเพิ่มพิสัยของข้อไหล่
Avoidance of pulling on the arm during
assist transfer
Pulmonary aspiration andpneumonia
Cause
* Dysphagia
* Poor cognitive function
Management
* Stimulation to increase arousal
* Close supervision of patient
* Swallowing training
* Chest PT
Psychosocial support
Patientmotivation
Family support : counseling, education
Post stroke depression : support, Coping
mechanism, Antidepressant, consult
psychiatrist
74.
9.ปัญหาด้านการสื่อความหมาย
Communication therapy
- Improve patient's ability to
speak, understand, write
- Improve quality of life
75.
GOAL
To improveability to speak , understand,
read & write.
To develop strategies that compensate for
circumvent speech & language problems.
To improve quality of life in minimizing
isolation.
In early stage ; help pt. establish a
reliable means for basic yes / no
communication.
Rehabilitation outcome
POSITIVE PREDICTORS
1. Family support
2. Bladder control in 1 - 2 wks
3. Proximal muscle recovery in 2 - 4 wks
4. Isolate pattern of muscles in 4 - 6 wks
5. Perception intact
6. Motivation, no depression
85.
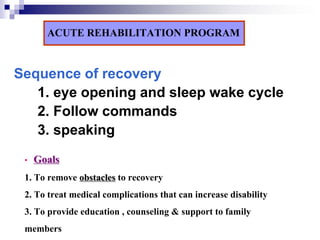
ACUTE REHABILITATION PROGRAM
Sequenceof recovery
1. eye opening and sleep wake cycle
2. Follow commands
3. speaking
• Goals
1. To remove obstacles to recovery
2. To treat medical complications that can increase disability
3. To provide education , counseling & support to family
members
86.
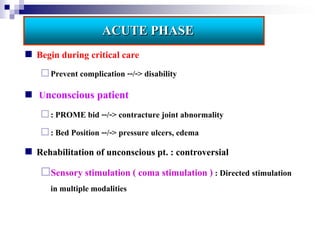
ACUTE PHASE
Begin during critical care
Prevent complication --/-> disability
Unconscious patient
: PROME bid --/-> contracture joint abnormality
: Bed Position --/-> pressure ulcers, edema
Rehabilitation of unconscious pt. : controversial
Sensory stimulation ( coma stimulation ) : Directed stimulation
in multiple modalities
87.
Physical impairment
Motor disturbances: most common
- disorders of balance and coordination
Increase muscle tone and contractures
- similar to spasticity associated with stroke
- Modified Ashworth Scale
Functional goals of spasticity treatment
-Improve hygiene -Decrease pain
-Decrease deformity -Improve orthotic fit
–Improve gait -Decrease energy expenditure of gait
-Facilitate motor control
88.
Reduce the levelof stimulation
Quiet private room
Remove noxious stimulation: tube, cath, restraints
Limit unnecessary sound: radio, TV
Limit no. of visitors and therapy sessions in room
Reduce pt’s cognitiveconfusion
. One person speaking to pt. at a time
. Maintain one staff to work
. Communicate to pt. briefly & simply
. Reorient pt. to place & time repeatedly