Downloaded 170 times





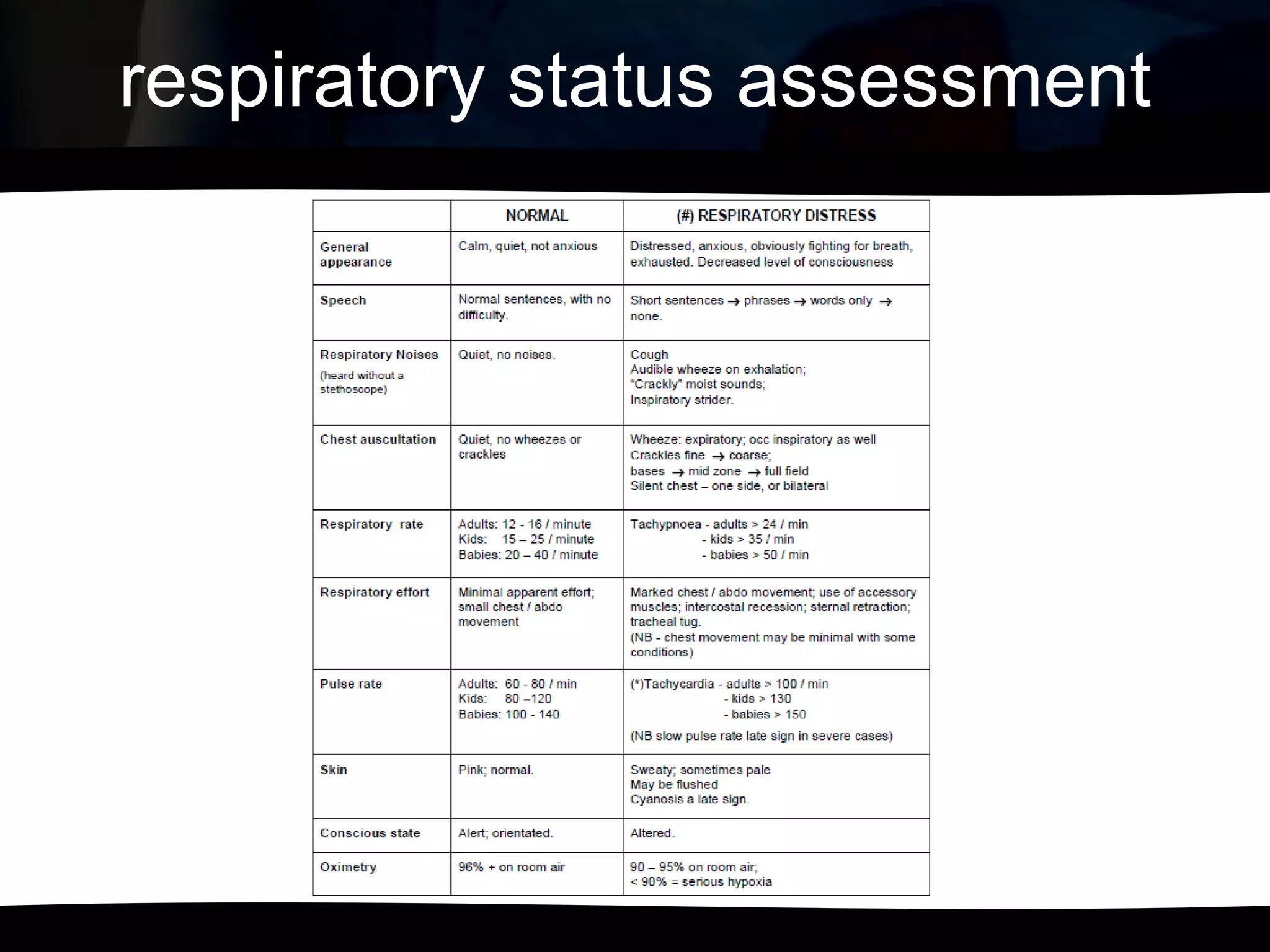

The document discusses signs of respiratory distress in children, including increased respiratory rate and effort of breathing, the use of accessory muscles, nasal flaring, and grunting. It describes how to assess respiratory status by examining respiratory rate, breath sounds, chest expansion, and pulse oximetry readings. The effects of respiratory inadequacy are described as pre-terminal signs like bradycardia, cyanosis, and unconsciousness. Various respiratory alterations and their management are also mentioned.






























































![Emergency Triage Assessment & ManagementETAT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cuetat1-241018195147-97d5df06-thumbnail.jpg?width=640&height=640&fit=bounds)
























