“Optimizing Chemoradiation Sequencing in Cervical Cancer”
1.
Optimizing the combinationor
sequencing of systemic therapies and
radiotherapy in carcinoma cervix
Dr Kanhu Charan Patro
MD,DNB(Radiation Oncology),MBA,FICRO,FAROI(USA),PDCR,CEPC
Clinical Director, HOD-Radiation Oncology
ISRo- Institute of Stereotactic Radiation oncology
Mahatma Gandhi Cancer Hospital & Research Institute, Visakhapatnam
drkcpatro@gmail.com /M- +91-9160470564/ www.drkanhupatro.com
2.
Dr. Kanhu CharanPatro
Clinical Director and HOD (Radiation Oncology)
(Brain Tumor Specialist)
Mahatma Gandhi Cancer Hospital & RI, Visakhapatnam
MBBS (Gold Medalist) MD, DNB (Radiation Oncology)
MBA (HA), FICRO, FAROI [USA], CEPC, PDCR
Visiting Fellow Manheim Cancer Center, Germany
Visiting trainee in Accuray Genolier, Switzerland
Visiting Fellow Well Cornell Medical College, New York
Ex. Resident (TMH-Mumbai) Visiting trainee (AIIMS-New Delhi)
drkcpatro@gmail.com / M-9160470564/drkanhupatro.com
SL SUBJECT INFERENCE
1 Area of interest NEURO AND URO-ONCOLOGY, NON - INVASIVE BRACHYTHERAPY
2 Clinical experience 25+ years
3 Cancer patients handled (RADIOTHERAPY) Nearly 10000
4 Brain tumors handled Nearly 900
5 Brachytherapy cases handled Nearly 4000
6 Interstitial brachytherapy cases handled Nearly 600
7 SRS/SBRT cases handled Nearly 200
8 Article publication Nearly 50
9 Slide share presentations Nearly 300
10 E Books/Chapter/Abstract Nearly 120
11 Awards received 12
12 Faculty invite- conferences More than 100
13 Thesis guided 10
14 Academic teacher experience 8 years
15 Fellowships awarded 4
11/03/2025 7
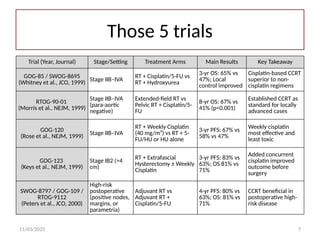
Those 5trials
Trial (Year, Journal) Stage/Setting Treatment Arms Main Results Key Takeaway
GOG-85 / SWOG-8695
(Whitney et al., JCO, 1999) Stage IIB–IVA
RT + Cisplatin/5-FU vs
RT + Hydroxyurea
3-yr OS: 65% vs
47%; Local
control improved
Cisplatin-based CCRT
superior to non-
cisplatin regimens
RTOG-90-01
(Morris et al., NEJM, 1999)
Stage IIB–IVA
(para-aortic
negative)
Extended-field RT vs
Pelvic RT + Cisplatin/5-
FU
8-yr OS: 67% vs
41% (p<0.001)
Established CCRT as
standard for locally
advanced cases
GOG-120
(Rose et al., NEJM, 1999)
Stage IIB–IVA
RT + Weekly Cisplatin
(40 mg/m²) vs RT + 5-
FU/HU or HU alone
3-yr PFS: 67% vs
58% vs 47%
Weekly cisplatin
most effective and
least toxic
GOG-123
(Keys et al., NEJM, 1999)
Stage IB2 (>4
cm)
RT + Extrafascial
Hysterectomy ± Weekly
Cisplatin
3-yr PFS: 83% vs
63%; OS 81% vs
71%
Added concurrent
cisplatin improved
outcome before
surgery
SWOG-8797 / GOG-109 /
RTOG-9112
(Peters et al., JCO, 2000)
High-risk
postoperative
(positive nodes,
margins, or
parametria)
Adjuvant RT vs
Adjuvant RT +
Cisplatin/5-FU
4-yr PFS: 80% vs
63%; OS: 81% vs
71%
CCRT beneficial in
postoperative high-
risk disease
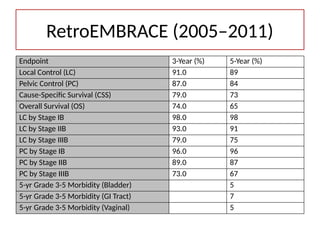
RetroEMBRACE (2005–2011)
• Design:Retrospective analysis of 731 patients
from 12 institutions
• Objective: Validate MRI-guided adaptive
brachytherapy outcomes
15.
RetroEMBRACE (2005–2011)
Endpoint 3-Year(%) 5-Year (%)
Local Control (LC) 91.0 89
Pelvic Control (PC) 87.0 84
Cause-Specific Survival (CSS) 79.0 73
Overall Survival (OS) 74.0 65
LC by Stage IB 98.0 98
LC by Stage IIB 93.0 91
LC by Stage IIIB 79.0 75
PC by Stage IB 96.0 96
PC by Stage IIB 89.0 87
PC by Stage IIIB 73.0 67
5-yr Grade 3-5 Morbidity (Bladder) 5
5-yr Grade 3-5 Morbidity (GI Tract) 7
5-yr Grade 3-5 Morbidity (Vaginal) 5
16.
Embrace I (2008)
•Design: International, multicenter, prospective
observational study
• Population: 1416 patients with cervical cancer
treated with MRI-guided adaptive brachytherapy
• Key Findings:
– Actuarial overall 5-year local control was 92%
– Improved outcomes compared with historical
controls
– Safety: acceptable late toxicity rates
Embrace II (Ongoing,since 2016)
• Design: International prospective study
building on Embrace I
• Aims
– Optimize image-guided brachytherapy Integrate
modern EBRT (IMRT/IGRT)
– Reduce morbidity while preserving efficacy
– Endpoints: Local control, progression-free survival,
quality of life, toxicity reduction
19.
Dose, Fractionation, Timing
•EBRT 45–50.4 Gy/25–28 fx with weekly
cisplatin
• Brachy: 4–5 fractions HDR; individualize per
HR CTV volume and OAR D2cc
‑
• Finish OTT ≤ 56 days; use workflow pathways
to avoid delays
20.
IMAGE GUIDED RADIATIONTHERAPY
EQUIPMENT REQUIRED
CT-SCAN MRI PET-CT
11/03/2025 20
Mahatma Gandhi Cancer Hospital &
Research Institute,Visakhapatnanm
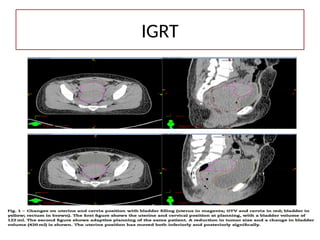
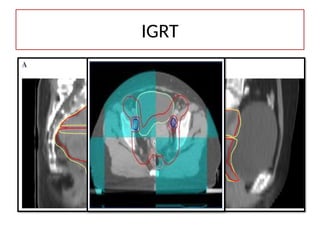
IGRT & AdaptiveEBRT
• Daily CBCT for set-up and organ filling
variations
• Re planning for tumor
‑
regression/bladder/rectum changes
• Consider offline/online adaptation in weeks 3–
4 if significant regression
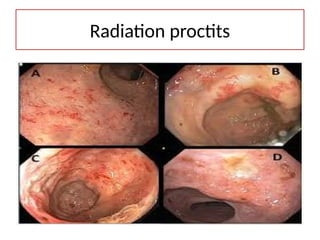
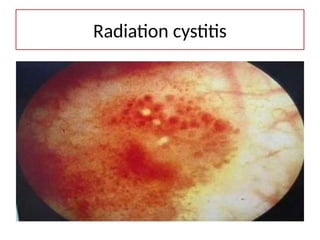
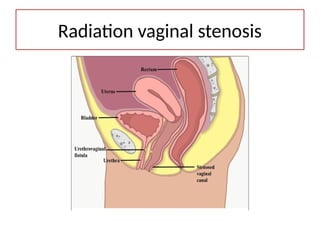
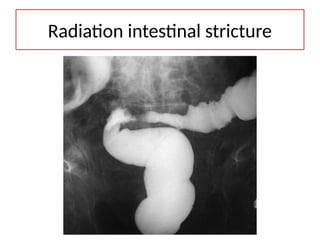
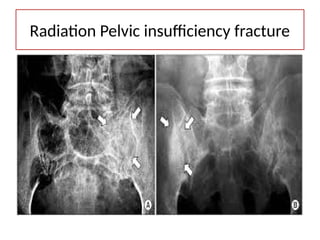
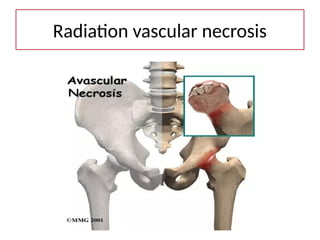
Radiation toxicity
• Bladderrelated
• Rectum related
• Bowel related
• Bone related
• Acute
• Late
11/03/2025 01:07:18 AM 37
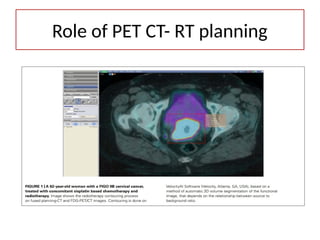
38.
Imaging to PlanWell
• Pelvic MRI for primary and parametria
• PET-CT for nodal staging
• Use MRI/CT for target delineation per
GEC ESTRO concepts (GTV, HR CTV, IR CTV)
‑ ‑ ‑
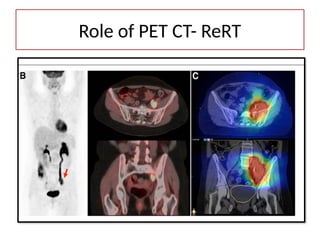
39.
Role of PETCT
When things are suspicious
PET CT is auspicious
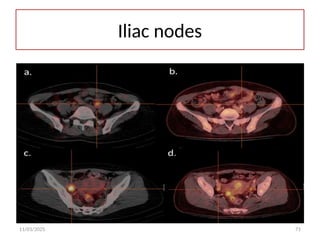
Identifying suspicious nodes
Boosting the nodes
Reirradiation settings
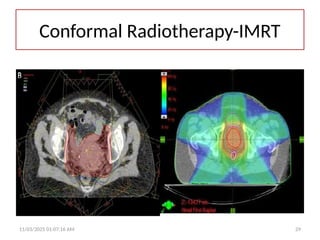
Why Advanced RTMatters
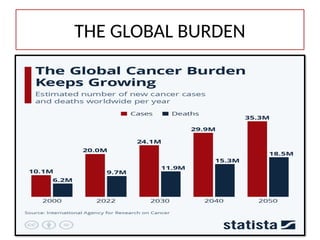
• High burden in LMICs; many present with
locally advanced disease
• Concurrent chemoradiation with
brachytherapy remains standard of care
• Advanced RT
– Improves local control
– Reduces toxicity vs. 2D plans
43.
11/03/2025 43
The defaultand standard sequence
• Concurrent chemoradiation with
cisplatin + brachytherapy, completed
within ~8 weeks.
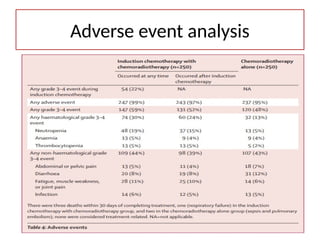
1. Higher hematologicaltoxicity in NACT arm (30% Grade 3–4 vs 13% in CTRT arm)
2. Main toxicities: Neutropenia (19% vs 5%), Anemia (28% vs 17%)
3. Non-hematological toxicities were similar between both groups
Toxicity
52.
• 3 deathswithin 30 days of completing
treatment, one (respiratory failure) in the
induction chemotherapy with
chemoradiotherapy group,
• 2 in the chemoradiotherapy alone group
(sepsis and pulmonary embolism); none were
considered treatment-related.
Death
53.
1. Temporary declinein QoL during
induction chemotherapy phase
2. No long-term differences between
the two groups after treatment
QOL
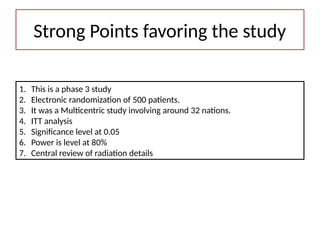
1. This isa phase 3 study
2. Electronic randomization of 500 patients.
3. It was a Multicentric study involving around 32 nations.
4. ITT analysis
5. Significance level at 0.05
6. Power is level at 80%
7. Central review of radiation details
Strong Points favoring the study
57.
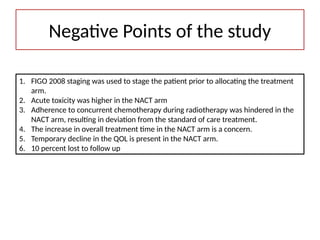
1. FIGO 2008staging was used to stage the patient prior to allocating the treatment
arm.
2. Acute toxicity was higher in the NACT arm
3. Adherence to concurrent chemotherapy during radiotherapy was hindered in the
NACT arm, resulting in deviation from the standard of care treatment.
4. The increase in overall treatment time in the NACT arm is a concern.
5. Temporary decline in the QOL is present in the NACT arm.
6. 10 percent lost to follow up
Negative Points of the study
11/03/2025 60
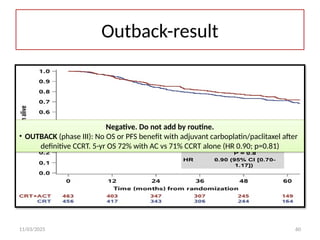
Outback-result
Negative. Donot add by routine.
• OUTBACK (phase III): No OS or PFS benefit with adjuvant carboplatin/paclitaxel after
definitive CCRT. 5-yr OS 72% with AC vs 71% CCRT alone (HR 0.90; p=0.81)
11/03/2025 65
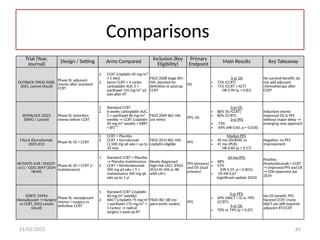
Comparisons
Trial (Year,
Journal)
Design/ Setting Arms Compared Inclusion (Key
Eligibility)
Primary
Endpoint
Main Results Key Takeaway
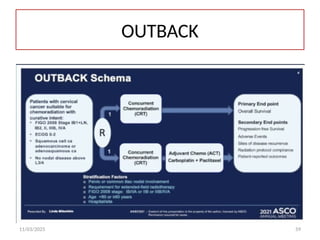
OUTBACK (TROG 0208,
2021, Lancet Oncol)
Phase III, adjuvant
chemo after standard
CCRT
1. CCRT (cisplatin 40 mg/m²
× 5 wks)
2. Same CCRT + 4 cycles
carboplatin AUC 5 +
paclitaxel 155 mg/m² q3
wks after RT
FIGO 2008 stage IB1–
IVA, planned for
definitive or post-op
CCRT
OS
5-yr OS
• 72% (CCRT)
• 71% (CCRT + ACT)
HR 0.90 (p = 0.81)
No survival benefit; do
not add adjuvant
chemotherapy after
CCRT
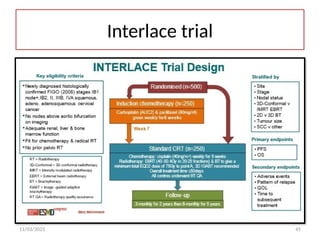
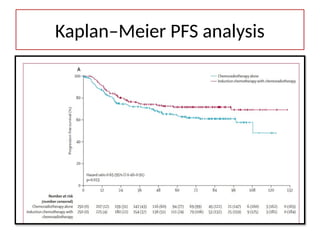
INTERLACE (2023
ESMO / Lancet)
Phase III, induction
chemo before CCRT
1. Standard CCRT
2. 6 weeks carboplatin AUC
2 + paclitaxel 80 mg/m²
weekly → CCRT (cisplatin
40 mg/m² weekly + EBRT
+ BT)**
FIGO 2009 IB2–IVA
(no mets)
PFS, OS
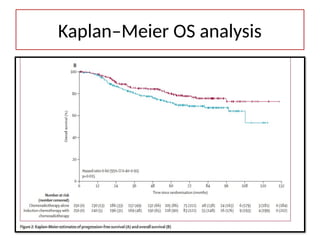
3-yr OS
• 86% (IC+CCRT)
• 80% (CCRT);
3-yr PFS
• 73%
• 64% (HR 0.65, p = 0.016)
Induction chemo
improved OS & PFS
without major delay →
emerging new approach
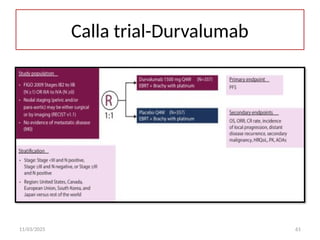
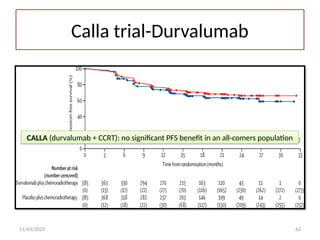
CALLA (Durvalumab,
2023 JCO)
Phase III, IO + CCRT
1. CCRT + Placebo
2. CCRT + Durvalumab
(1,500 mg q4 wks × up to
24 mo)
FIGO 2014 IB2–IVA;
cisplatin eligible
PFS
Median PFS
• 40 mo (DURVA) vs
• 41 mo (PLB);
HR 0.84 (p = 0.17)
Negative; no PFS
improvement
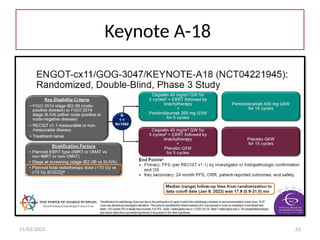
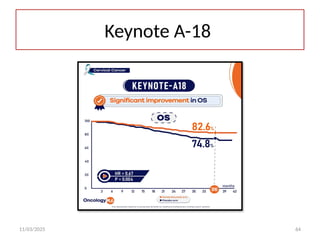
KEYNOTE-A18 / ENGOT-
cx11 / GOG-3047 (2024
NEJM)
Phase III, IO + CCRT (+
maintenance)
1. Standard CCRT + Placebo
→ Placebo maintenance
2. CCRT + Pembrolizumab
200 mg q3 wks × 5 +
maintenance 400 mg q6
wks up to 1 yr
Newly diagnosed
high-risk LACC (FIGO
2014 III–IVA or IIB
with LN+)
PFS (primary)
and OS (dual
primary)
24-mo PFS
• 68%
• 57%
(HR 0.59, p < 0.001);
• OS HR 0.67
(significant update 2024)
Positive;
Pembrolizumab + CCRT
→ improved PFS and OS
→ FDA-approved Jan
2024
EORTC 55994
(Neoadjuvant → Surgery
vs CCRT, 2022 Lancet
Oncol)
Phase III, neoadjuvant
chemo + surgery vs
definitive CCRT
1. Standard CCRT (cisplatin
40 mg/m² weekly)
2. NACT (cisplatin 75 mg/m²
+ paclitaxel 175 mg/m² ×
3 cycles) → radical
surgery ± post-op RT
FIGO IB2–IIB (no
para-aortic nodes)
PFS
5-yr PFS
• 69% (NACT + S) vs 76%
(CCRT);
5-yr OS
• 76% vs 74% (p = 0.67)
No OS benefit; PFS
favored CCRT; many
NACT pts still required
adjuvant RT/CCRT
66.
11/03/2025 66
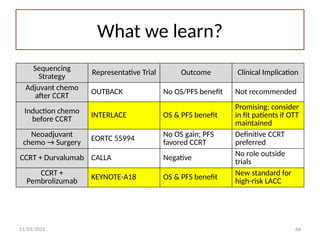
What welearn?
Sequencing
Strategy
Representative Trial Outcome Clinical Implication
Adjuvant chemo
after CCRT
OUTBACK No OS/PFS benefit Not recommended
Induction chemo
before CCRT
INTERLACE OS & PFS benefit
Promising; consider
in fit patients if OTT
maintained
Neoadjuvant
chemo → Surgery
EORTC 55994
No OS gain; PFS
favored CCRT
Definitive CCRT
preferred
CCRT + Durvalumab CALLA Negative
No role outside
trials
CCRT +
Pembrolizumab
KEYNOTE-A18 OS & PFS benefit New standard for
high-risk LACC
67.
11/03/2025 67
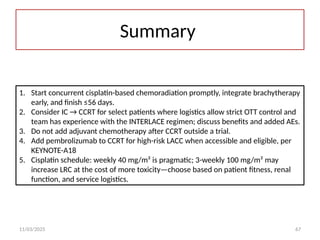
Summary
1. Startconcurrent cisplatin-based chemoradiation promptly, integrate brachytherapy
early, and finish ≤56 days.
2. Consider IC → CCRT for select patients where logistics allow strict OTT control and
team has experience with the INTERLACE regimen; discuss benefits and added AEs.
3. Do not add adjuvant chemotherapy after CCRT outside a trial.
4. Add pembrolizumab to CCRT for high-risk LACC when accessible and eligible, per
KEYNOTE-A18
5. Cisplatin schedule: weekly 40 mg/m² is pragmatic; 3-weekly 100 mg/m² may
increase LRC at the cost of more toxicity—choose based on patient fitness, renal
function, and service logistics.
11/03/2025 75
Adenocarcinoma –Needof adjuvant?
1. Adenocarcinoma of the cervix does not automatically
mandate more aggressive adjuvant chemotherapy after CCRT,
in the absence of other high-risk factors.
2. However, given its biologic behavior (often higher risk of
distant relapse), you should be more vigilant, assess risk
carefully, and have a low threshold for multi-disciplinary
discussion.
3. Optimize the core CCRT delivery first; if high-risk features are
present, adjuvant chemo can be considered on a case-by-case
basis.
4. Document the discussion, involve the patient in decision-
making, and monitor outcomes carefully
76.
11/03/2025 76
TAKE HOMEMESSAGE
• Concurrent CTRT is the standard
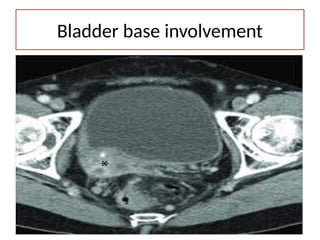
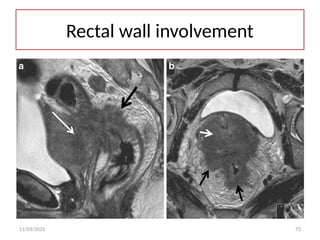
• Prefer NACT in large nodes and bladder and
rectal wall involvement
• Consider adjuvant chemo in adenocarcinoma
• Immunotherapy not the standard yet can be
considered in patient is affordable.
• Consider adjuvant chemo in adenocarcinoma
variant.{very low level-evidence}
77.
Thank you
DOWNLOAD ONCOEDUCATIONAPP
Simplified and Comprehensive
Oncology Education and
Prevention
PPTS,OSCE,
SHORT NOTES etc.
No SCOPE to fail

![Dr. Kanhu Charan Patro
Clinical Director and HOD (Radiation Oncology)
(Brain Tumor Specialist)
Mahatma Gandhi Cancer Hospital & RI, Visakhapatnam
MBBS (Gold Medalist) MD, DNB (Radiation Oncology)
MBA (HA), FICRO, FAROI [USA], CEPC, PDCR
Visiting Fellow Manheim Cancer Center, Germany
Visiting trainee in Accuray Genolier, Switzerland
Visiting Fellow Well Cornell Medical College, New York
Ex. Resident (TMH-Mumbai) Visiting trainee (AIIMS-New Delhi)
drkcpatro@gmail.com / M-9160470564/drkanhupatro.com
SL SUBJECT INFERENCE
1 Area of interest NEURO AND URO-ONCOLOGY, NON - INVASIVE BRACHYTHERAPY
2 Clinical experience 25+ years
3 Cancer patients handled (RADIOTHERAPY) Nearly 10000
4 Brain tumors handled Nearly 900
5 Brachytherapy cases handled Nearly 4000
6 Interstitial brachytherapy cases handled Nearly 600
7 SRS/SBRT cases handled Nearly 200
8 Article publication Nearly 50
9 Slide share presentations Nearly 300
10 E Books/Chapter/Abstract Nearly 120
11 Awards received 12
12 Faculty invite- conferences More than 100
13 Thesis guided 10
14 Academic teacher experience 8 years
15 Fellowships awarded 4](https://image.slidesharecdn.com/ctrtsequencingincancercervix-251103010701-18b465a1/85/Optimizing-Chemoradiation-Sequencing-in-Cervical-Cancer-2-320.jpg)









![management of advanced cervical cancer [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/managementofadvancedcervicalcancerautosaved-230926014710-62f747b3-thumbnail.jpg?width=640&height=640&fit=bounds)





















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









