Downloaded 161 times

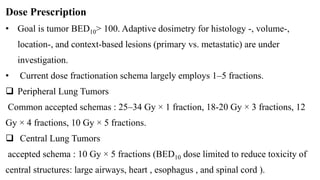
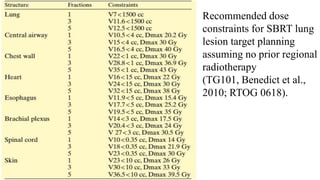
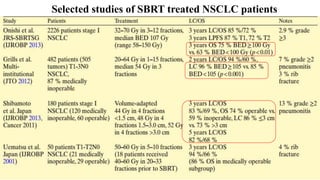





This document discusses lung stereotactic body radiotherapy (SBRT) for the treatment of early stage non-small cell lung cancer (NSCLC). It covers treatment indications for SBRT, methods used to account for tumor motion including 4DCT planning and respiratory gating, treatment planning guidelines, evidence from studies showing high rates of local control and survival, and results from RTOG trials of SBRT for lung cancer. In particular, it highlights that SBRT achieves local control rates of 85-95% and overall survival rates of 50-95% at 3-5 years for early stage NSCLC.



















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















