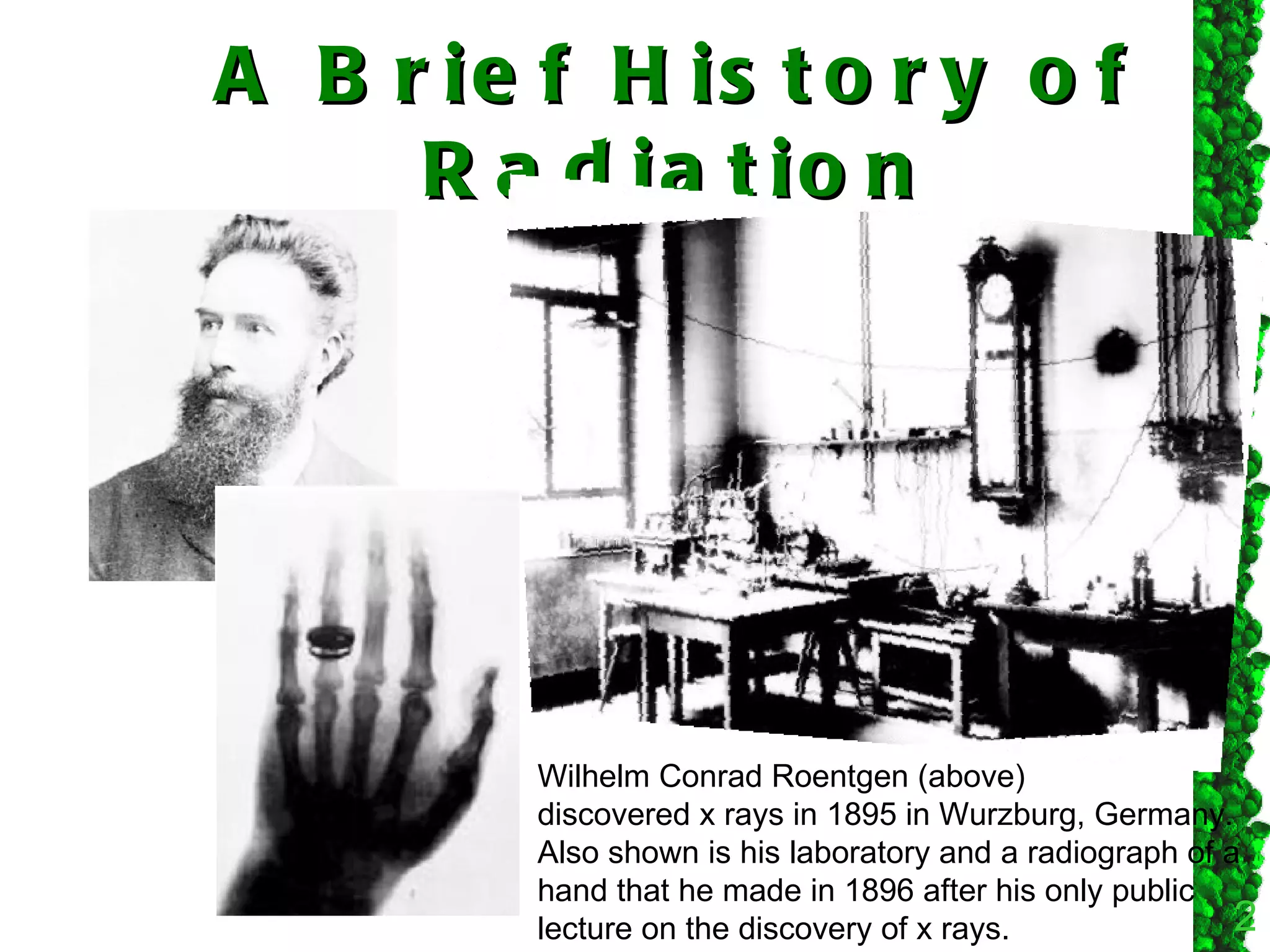
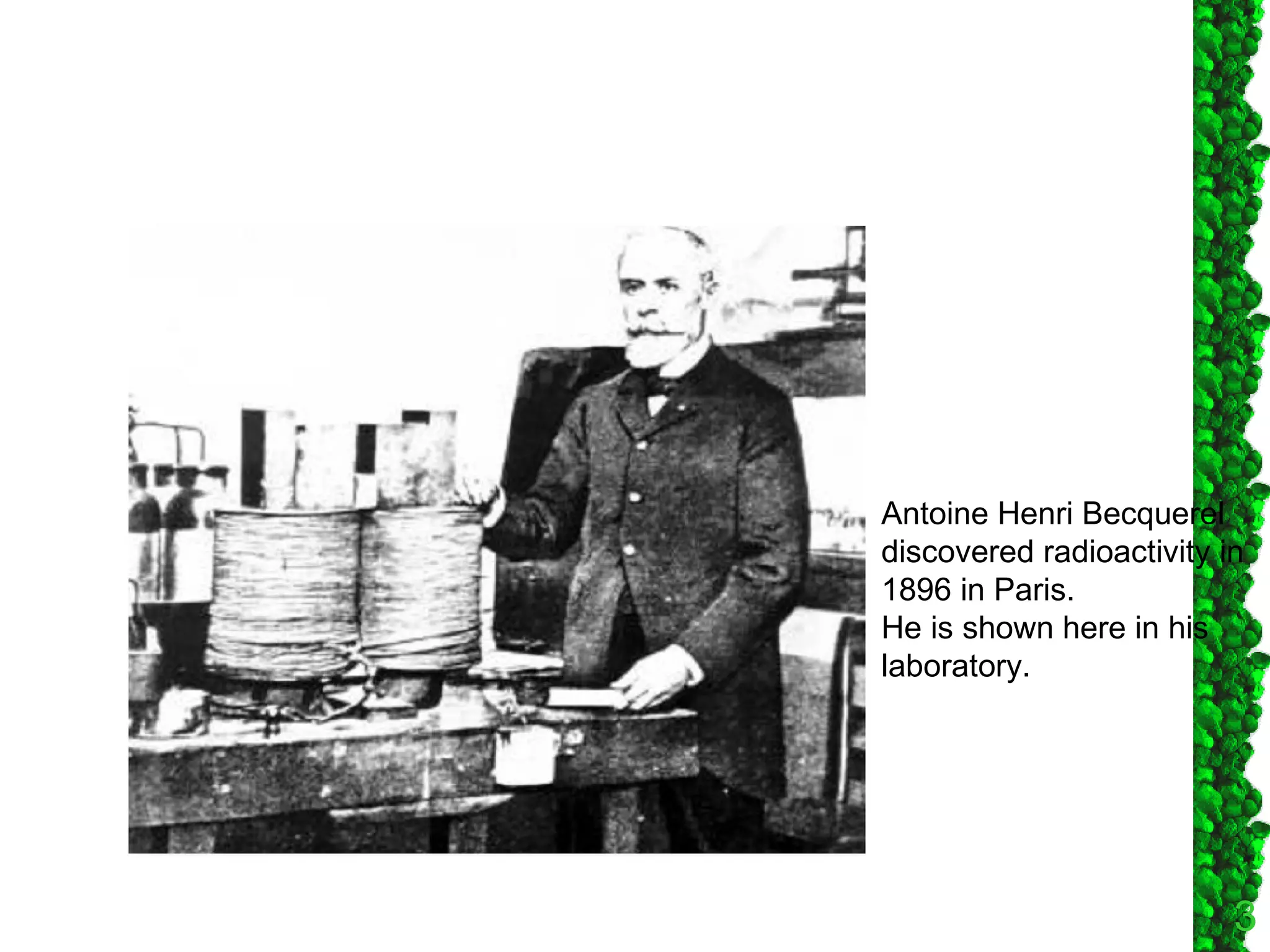
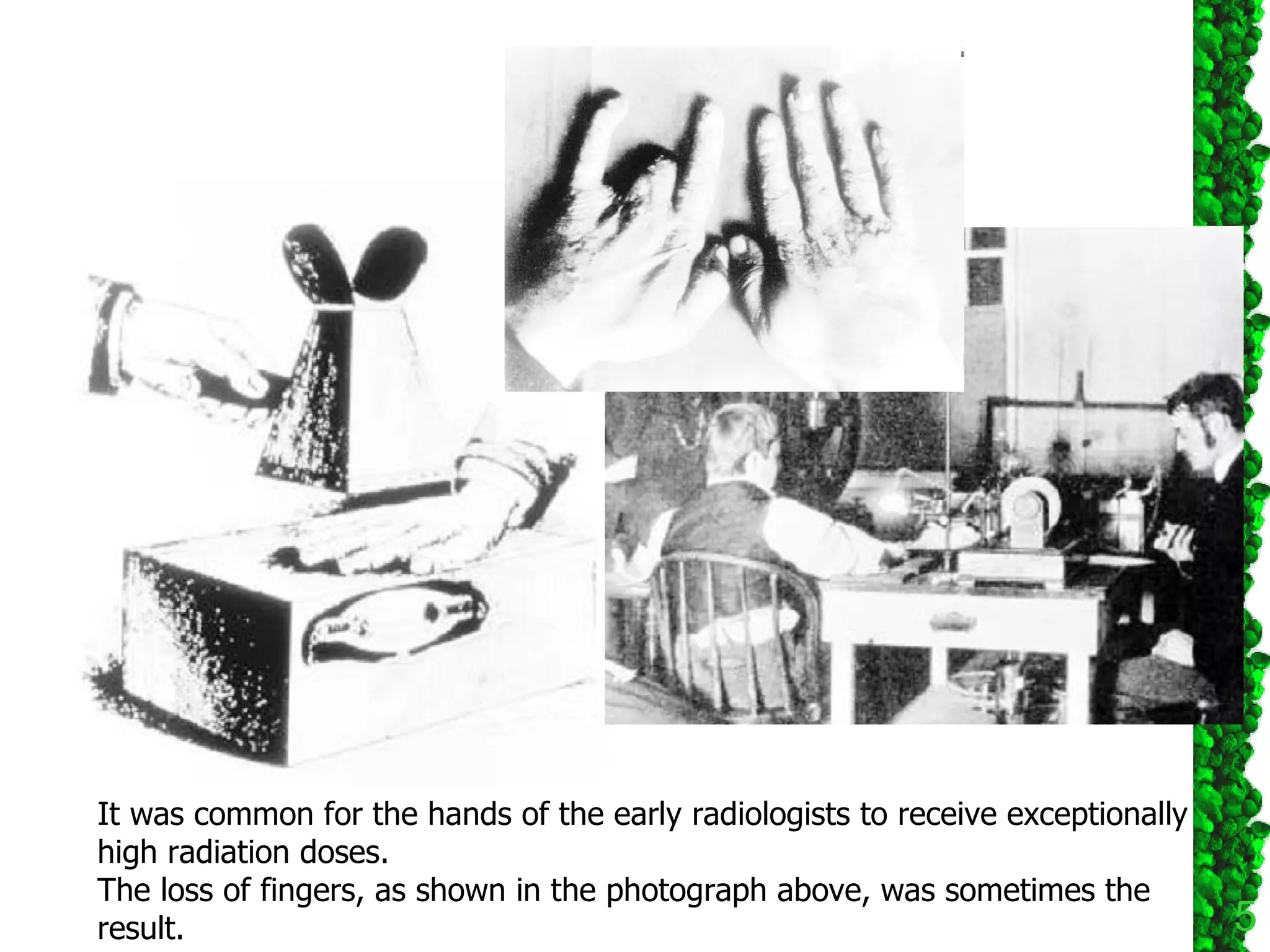




The document discusses the evolution of radiation dose standards over time from the discovery of x-rays in 1895. Early researchers did not understand the biological effects of radiation and suffered injuries. Formal standards began in the early 1900s and continued to be refined through the 1900s based on new research findings. The standards set limits on radiation exposure for occupational workers and the general public based on balancing radiation risks and the benefits of practices involving radiation sources.






























































































