Downloaded 135 times
























![ICRP103 provided detailed explanations of the bases for the choice of
WR values based on mixture of Science and Pragmatism
New Recommendations : ICRP 103
Contd……
Radiation Type Radiation Weighting
Factor (WR) based on
ICRP 103
Radiation Weighting Factor (WR)
based on ICRP 60
Photons, Electrons &
Muons
1 1
Protons & Charged
Pions
2 5
Alpha particles, fission
fragments, heavy ions
20 20
Neutrons Continuous function of
neutron energy
˂1 MeV 2.5+18.2 e-[ln(E)2]/6
1 to 50 MeV 5.0+17.0 e-[ln(2E)]2/6
˃50 MeV 2.5+3.25 e-[ln(0.04 E)2]/6
Note: WR for Neutron is a continuous function instead of step function](https://image.slidesharecdn.com/icrp60-171226165236/85/Icrp60-27-320.jpg)
















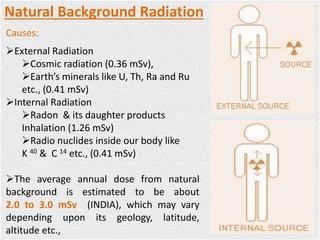
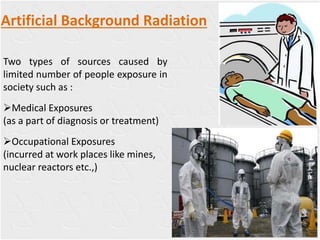
The document discusses recommendations from ICRP 60 & 103 regarding radiation protection. It begins with background on natural and artificial radiation sources and their effects. It then summarizes the evolution of ICRP recommendations over time, from early annual dose limits of 1000 mSv reduced gradually to current limits. Key concepts discussed include justification of practices, optimization of protection, and application of dose limits. Occupational, public, and medical exposure dose limits are provided. ICRP 103 introduced changes like new tissue weighting factors and computational phantoms.











































































