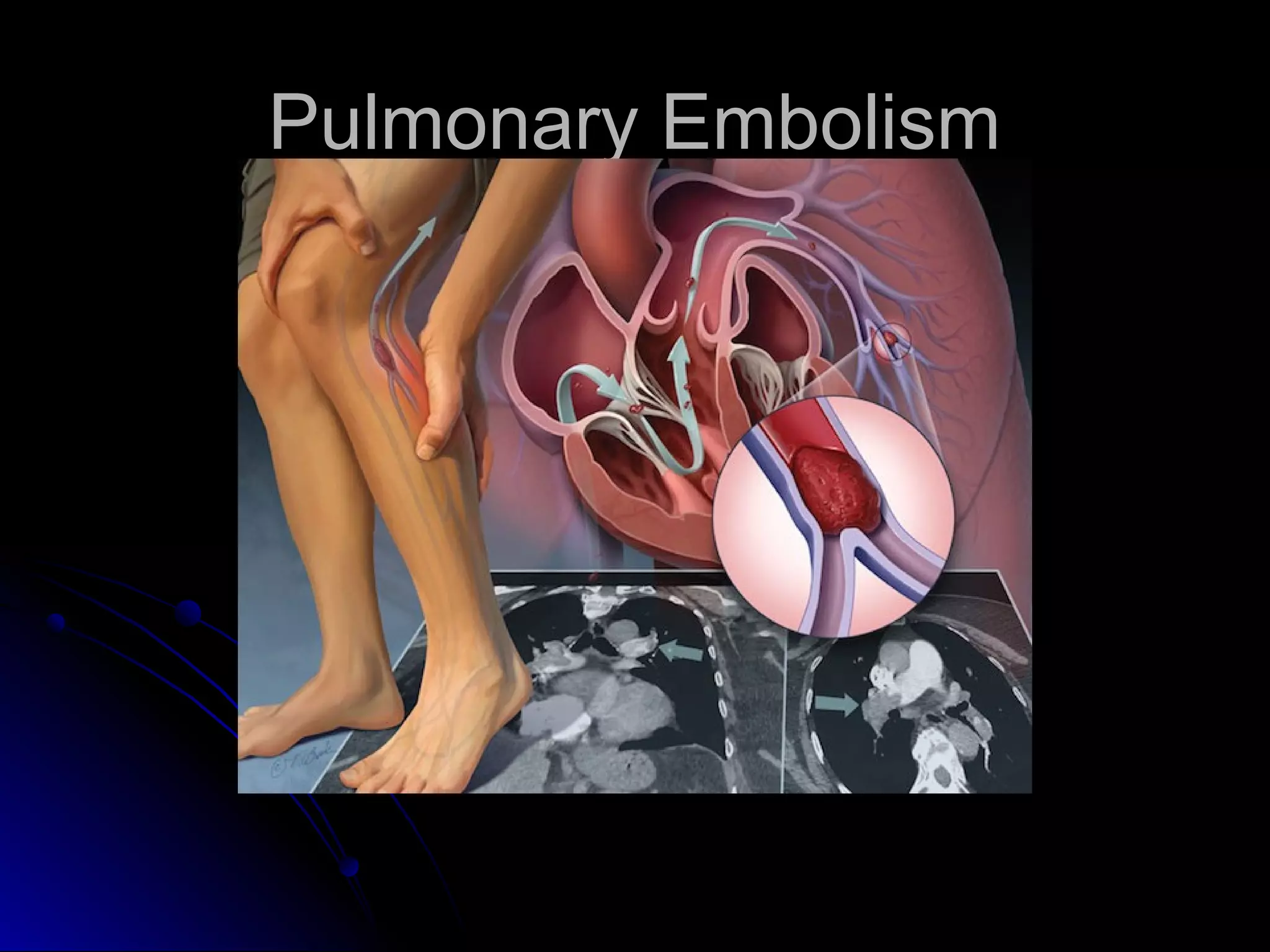
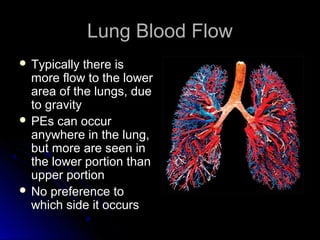
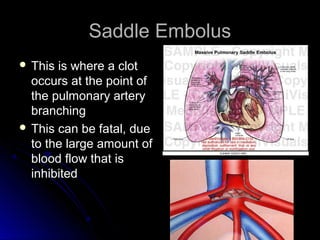
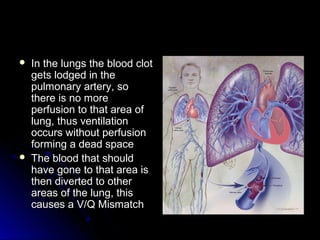
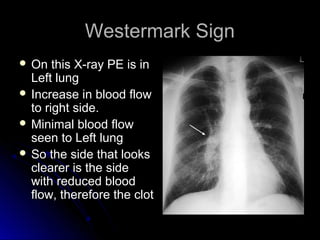
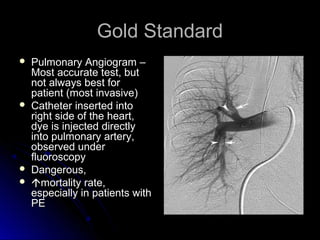
The document discusses pulmonary embolism (PE), including its causes, diagnosis, risk factors, and treatment. It highlights the process by which blood clots from the venous system can travel to the lungs and cause serious complications. Various diagnostic methods, including imaging techniques and tests such as D-dimer and ultrasound, are outlined, along with the symptoms and potential indicators associated with PE.




![Alveolar-arterial oxygen (A-a)Alveolar-arterial oxygen (A-a)
gradientgradient
PPAAOO22 - P- PaaOO22 should equal (Age (years) / 4) + 4should equal (Age (years) / 4) + 4
PPAAOO22 = [(F= [(FiiOO22) x (760 – 47)] – (P) x (760 – 47)] – (PaaCOCO22 / 0.8)/ 0.8)
Barometric Pressure = 760mmHgBarometric Pressure = 760mmHg
Water Vapour Pressure = 47mmHgWater Vapour Pressure = 47mmHg
Respiratory Coefficient = 0.8Respiratory Coefficient = 0.8
UseUsePPaaOO22 andandPPaaCOCO22 in mmHg not KPain mmHg not KPa
Eg 40 Yr old,Eg 40 Yr old,
FFiiOO22 0.60.6
PPaaCOCO22 32.5 mmHg32.5 mmHg (4.27KPa)(4.27KPa)
PPaaOO22 65 mmHg (8.55KPa)65 mmHg (8.55KPa)
PPAAOO22 =(0.6 x 713) – 40.6 = 387.2=(0.6 x 713) – 40.6 = 387.2
PPAAOO22 - P- PaaOO22 = 387.2 – 65 = 322.2= 387.2 – 65 = 322.2
(40/4) = 10 (+4) = 14(40/4) = 10 (+4) = 14
Therefore 322.2 > 14Therefore 322.2 > 14
So if the A-a gradient > 14 it may be indicative of a PESo if the A-a gradient > 14 it may be indicative of a PE](https://image.slidesharecdn.com/pulmonaryembolism-150816110059-lva1-app6891/85/Pulmonary-Embolism-PE-15-320.jpg)










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










