Download as PDF, PPTX
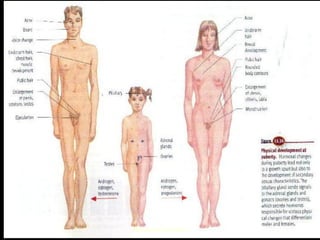




1. Puberty is defined as the transitional stage from childhood to adulthood that is characterized by physiological changes and development of secondary sex characteristics. 2. It typically occurs between ages 10-16 and is influenced by genetic and environmental factors such as nutrition, geography, and light exposure. 3. The stages of puberty include thelarche, adrenarche, growth spurt, menarche, and development of secondary sex characteristics over approximately 4.5 years.



























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















