Downloaded 161 times





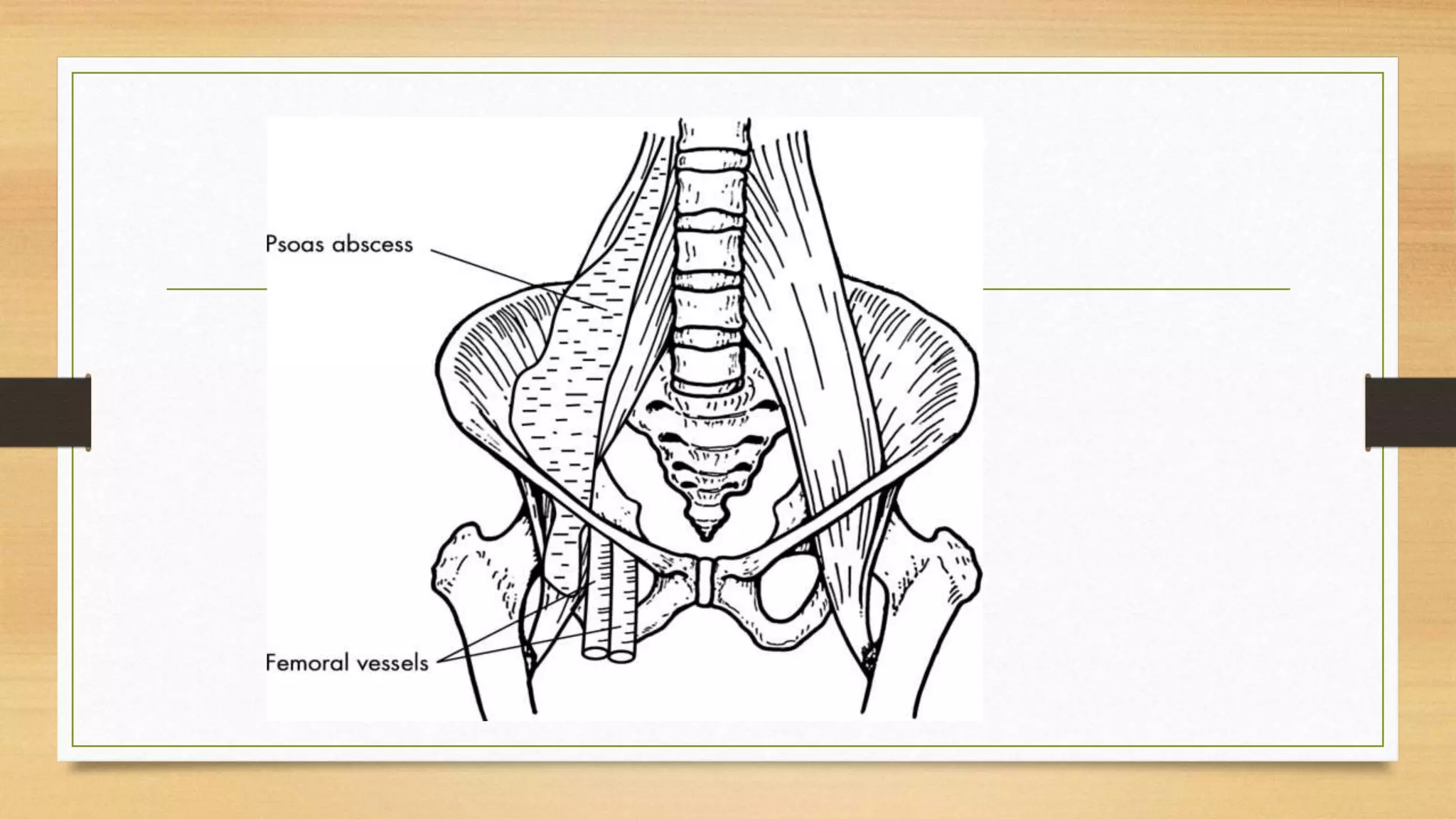



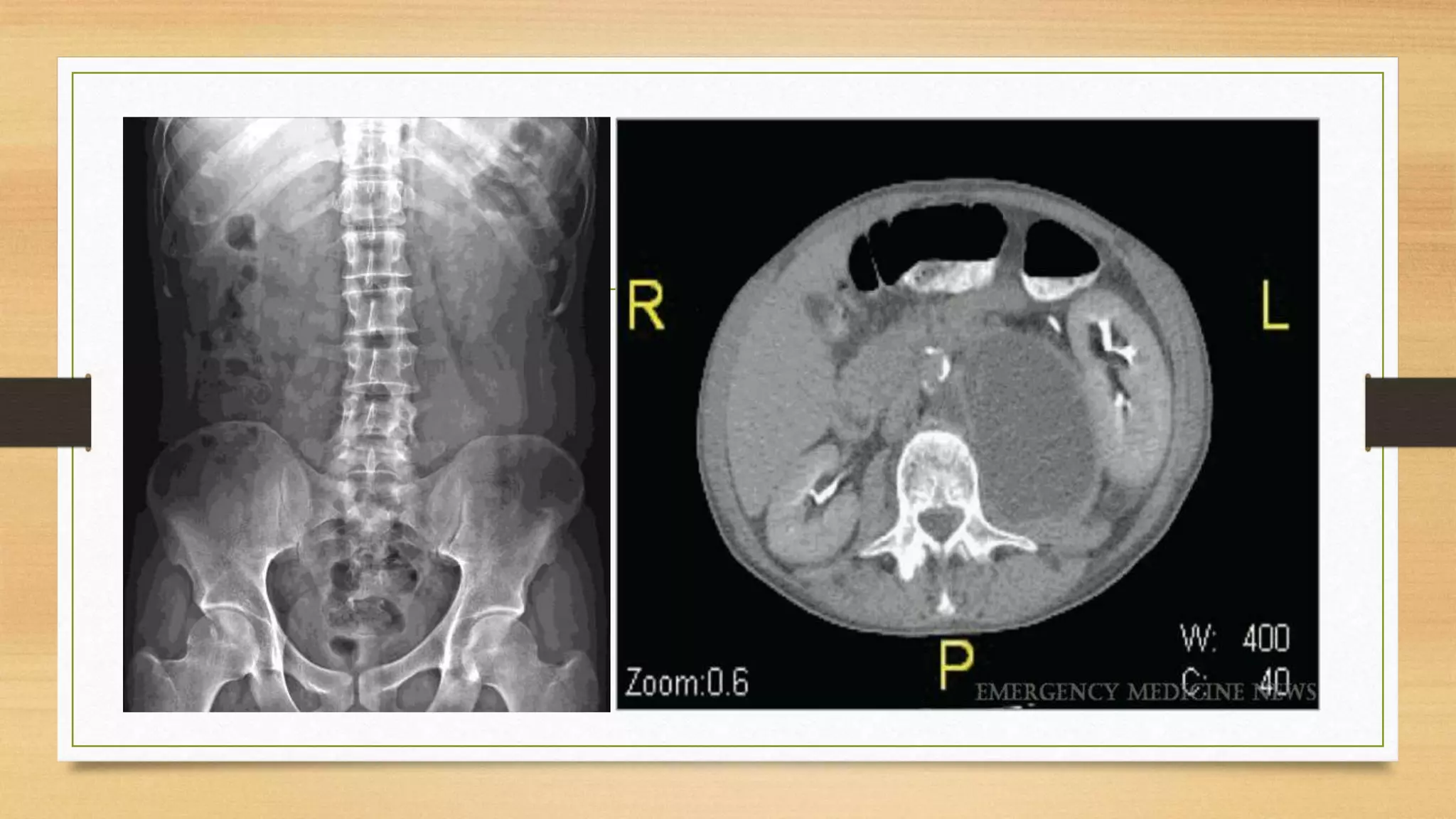
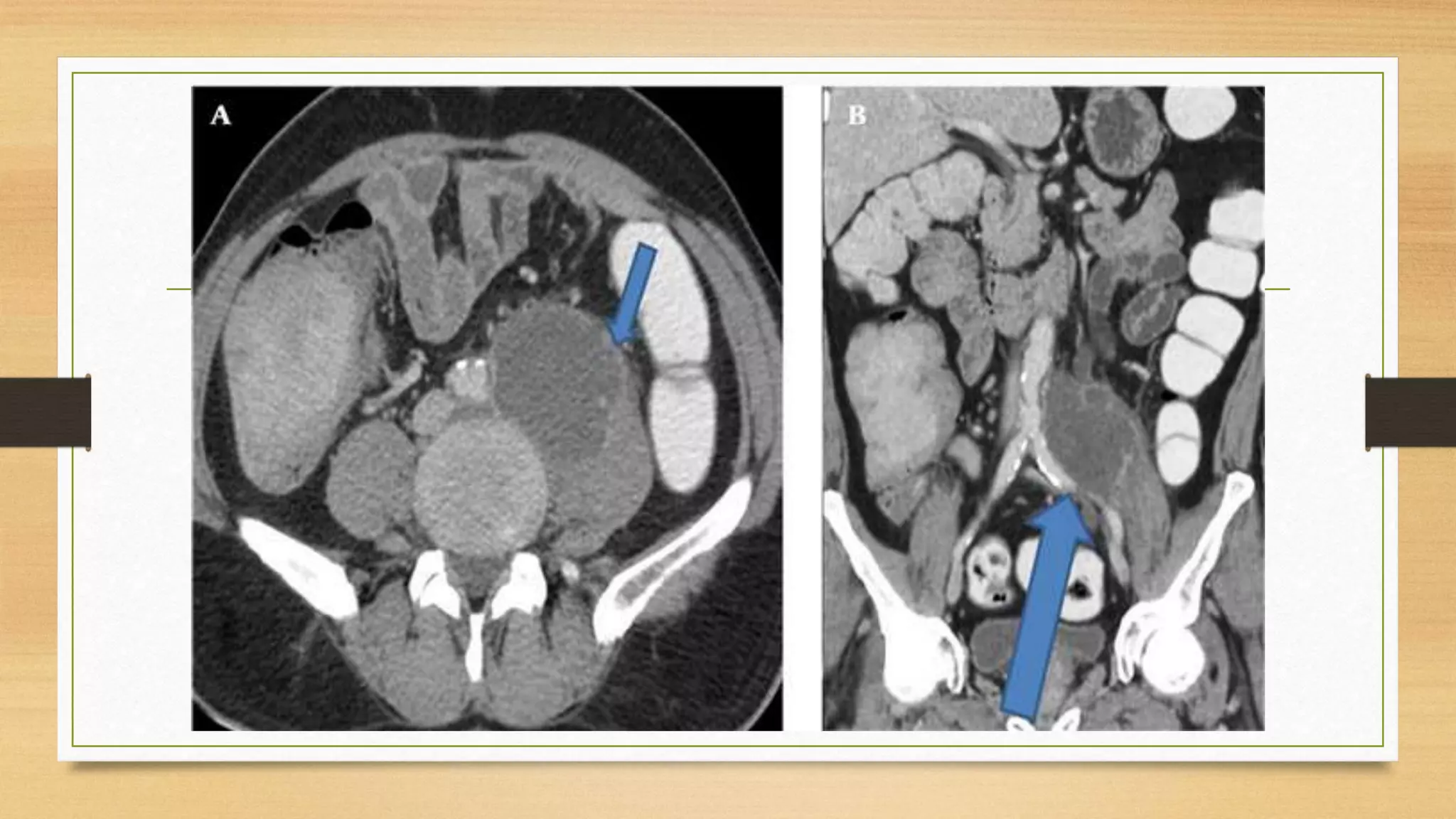








1. Psoas abscess is a collection of pus within the psoas muscle compartment. It can be primary, from hematogenous spread in immunocompromised patients, or secondary from adjacent organ infections like the spine, kidneys, or GI tract. 2. Clinical features include abdominal or flank pain, fever, and a limp. Examination may reveal pain with hip extension or leg lifting. Imaging like CT or MRI can confirm the hypodense lesion. 3. Treatment involves antibiotics based on culture results as well as surgical drainage of the abscess through approaches like the lateral loin or anterior incision.



































































