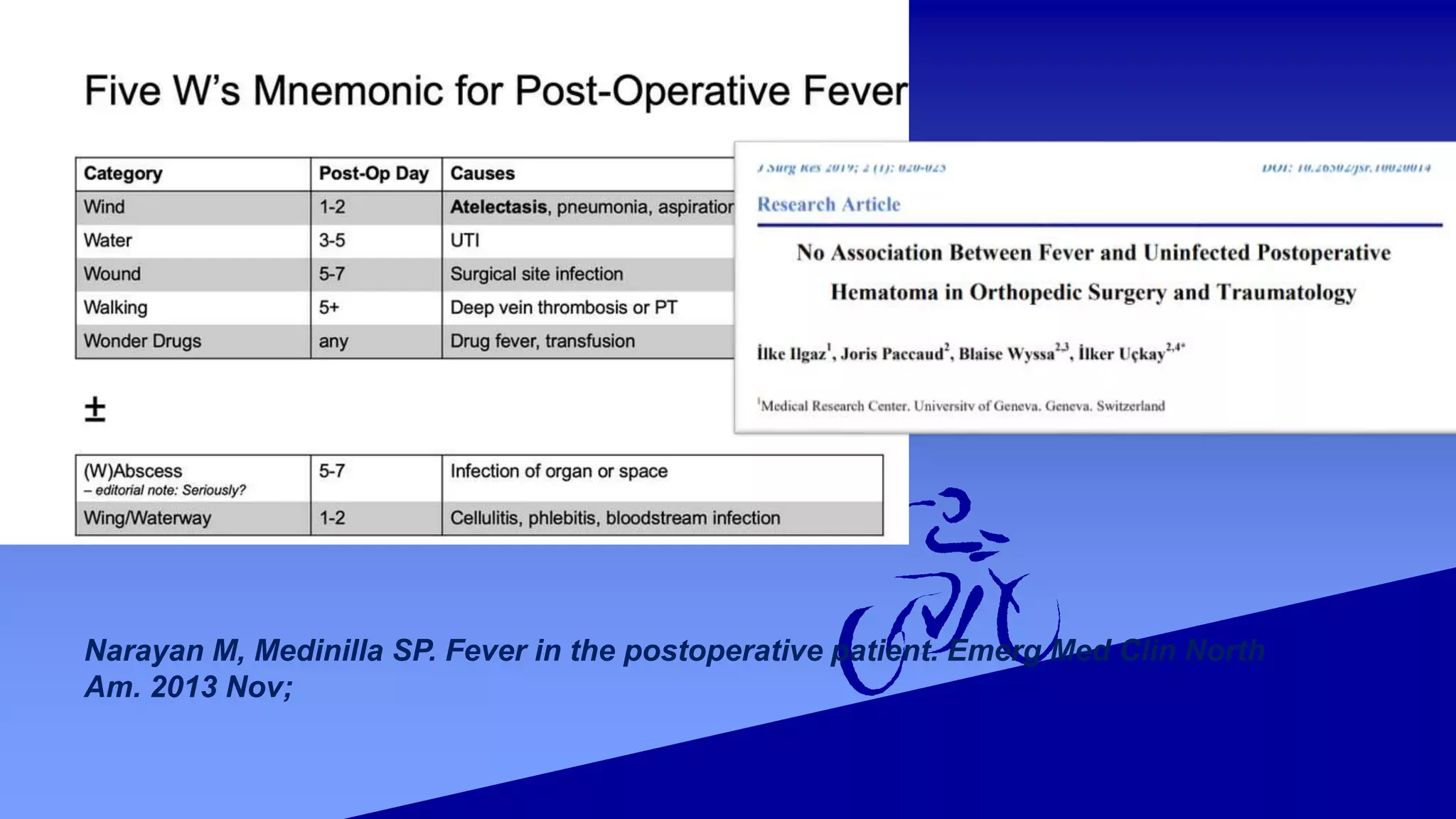
This document discusses postoperative fever, defining it as a temperature above 38°C or 39°C on consecutive or any postoperative days, respectively. It describes the pathophysiology of fever as an inflammatory response to surgery rather than necessarily indicating infection. It outlines criteria for systemic inflammatory response syndrome (SIRS) and discusses various potential causes of immediate, acute, subacute, and delayed postoperative fevers. Evaluation involves assessing vital signs, examination of wounds/lines/tubes, and ordering relevant labs and imaging. Treatment focuses on identifying and removing infection sources, providing IV fluids and antibiotics as needed. The take-home points are that fever alone does not prove infection and may resolve spontaneously within a week after surgery.